Downloaded 240 times





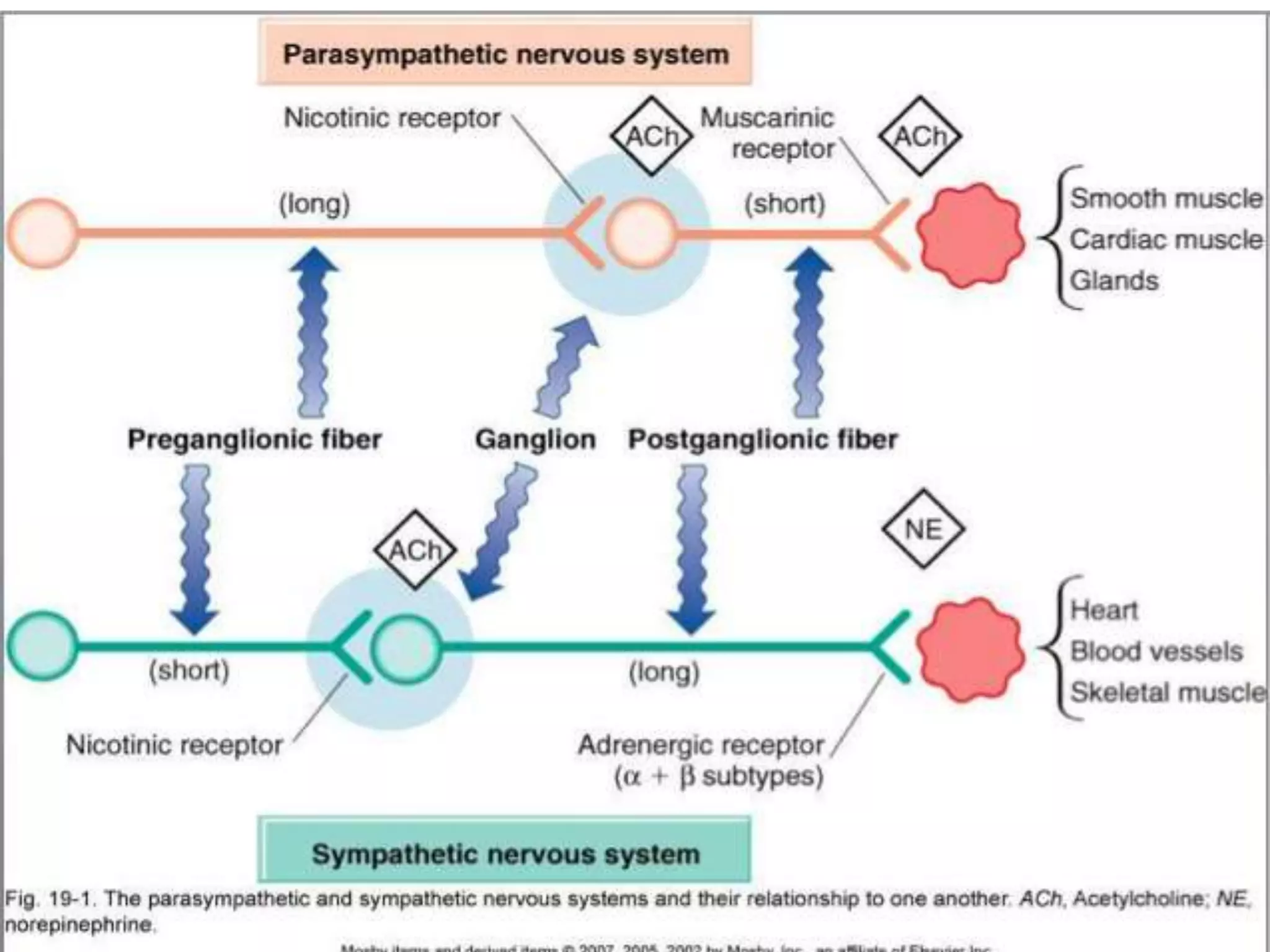


























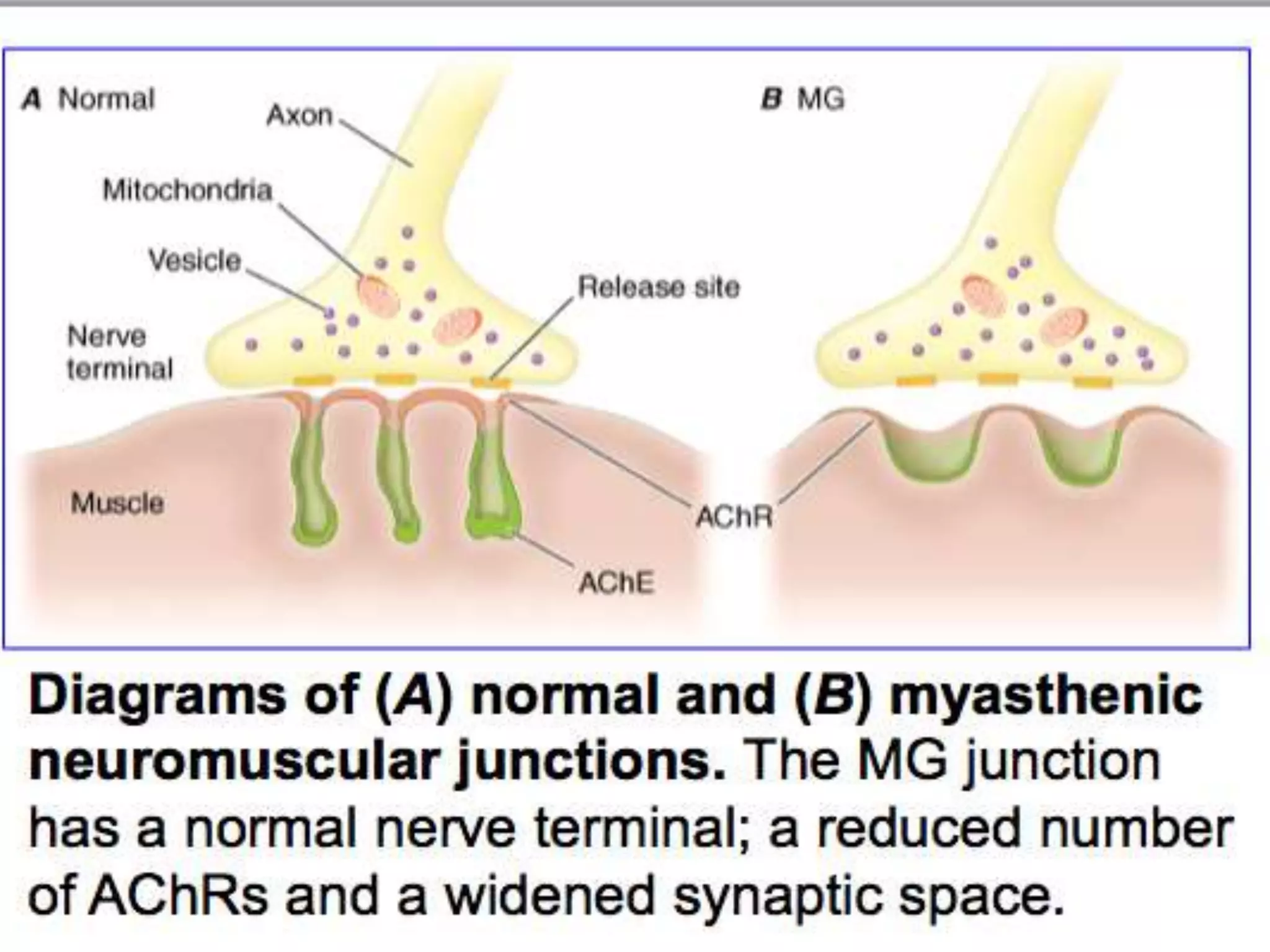













This document discusses the autonomic nervous system (ANS) and cholinergic drugs. It begins by describing the ANS and its role in regulating vital functions. Acetylcholine is the primary neurotransmitter of the parasympathetic nervous system. Cholinergic drugs such as acetylcholine esters and anticholinesterases work by increasing acetylcholine levels in the body. Anticholinesterases inhibit the acetylcholinesterase enzyme, preventing the breakdown of acetylcholine. These drugs have applications in conditions like glaucoma, Alzheimer's disease, and myasthenia gravis.






















































































