Downloaded 65 times







![8
Simple frenum with anodule [Figure 5]
Simple frenum with appendix [Figure 6]
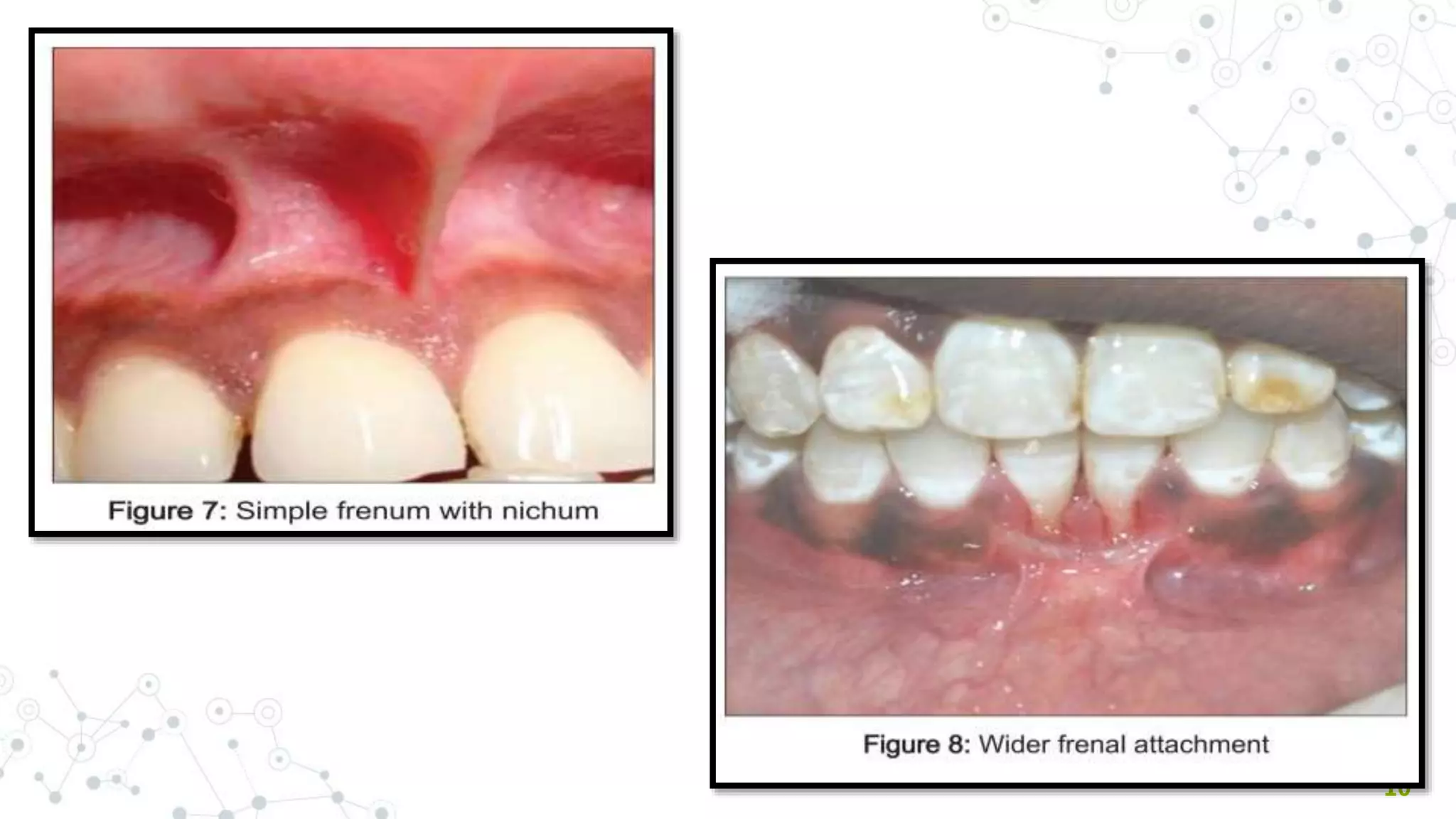
Simple frenum with nichum [Figure 7]
Bifid labial frenum
Persistent tectolabial frenum
Double frenum
Wider frenum [Figure 8]
Frenum with two or more variations at the same time
Sewerin’s Classification ( Based on morphotypes)
Other variations of normal frenal attachment
include:](https://image.slidesharecdn.com/frenumppt-210529174920/75/FRENAL-ATTACHMENT-ITS-MANAGEMENT-8-2048.jpg)






















































This document discusses frena, their development and classifications. It describes abnormal frenal attachments and their associated complications like loss of papilla and recession. Ankyloglossia (tongue-tie) is discussed in detail along with its classification and clinical features. Various techniques for treating abnormal frena are presented, including frenectomy, frenotomy, Z-plasty and laser frenectomy. Post-operative instructions are provided. The document emphasizes that proper technique selection based on frenal attachment type can achieve functional and aesthetic outcomes.
Introduction to frenum and its management, including contents overview.
Definition of frenum, its development, and primary functions in oral stability.
Classification of frena based on attachment types and morphological variations.
Tests and methods for diagnosing abnormal frenal attachments and their implications.
Issues arising from abnormal frenum attachments, including periodontal implications.
Syndromes associated with abnormal frenal attachments, discussing genetic disorders.
Introduction to ankyloglossia (tongue-tie) and its impact on speech articulation.
Classification of ankyloglossia into four classes based on the length of the lingual frenum.
Developmental origins of ankyloglossia due to improper tongue release during growth.
Clinical complications of ankyloglossia, including limitations in mobility and feeding issues.
Methods for treating ankyloglossia, including frenotomy and frenectomy.
Different surgical techniques for frenectomy, highlighting traditional approaches.
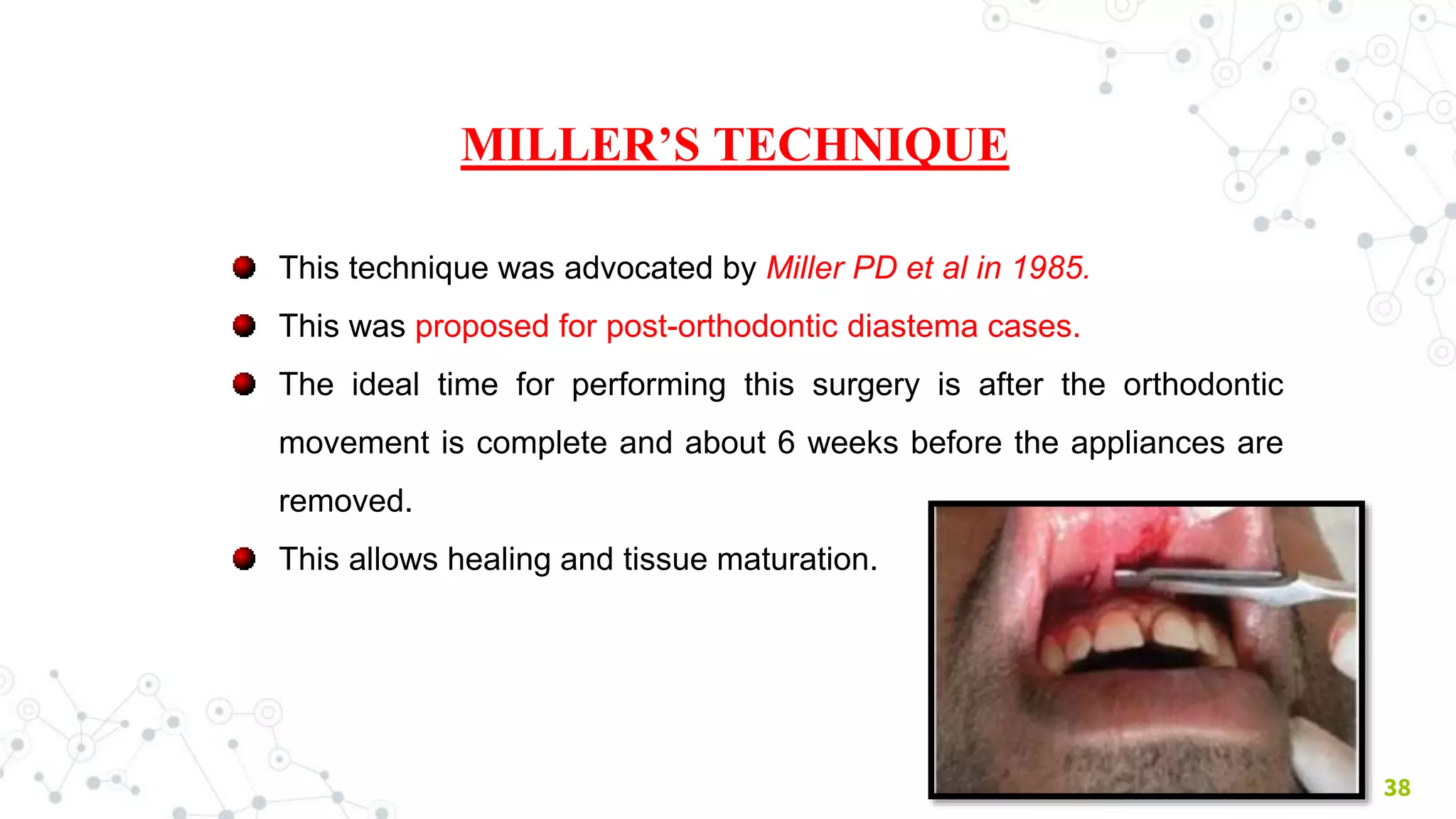
Benefits of Miller's technique and its effect on orthodontic outcomes.
Technique and indications for Z-plasty to correct frenal attachment issues.
Describing the V-Y plasty technique and its application in frenal surgeries.
Advantages of using electrosurgery techniques for frenectomy procedures.
Exploring benefits of laser frenectomy, including reduced recovery time.
Guidelines for post-operative care after frenectomy surgery.
Concluding remarks on the importance of assessing and treating abnormal frenal attachments.
Citations and references supporting the information presented in the slides.
















































































