Downloaded 72 times










































The document describes India's Integrated Disease Surveillance Project (IDSP), which aims to establish a decentralized, district-based system for surveillance of communicable and non-communicable diseases. Key elements of IDSP include integrating existing surveillance activities, strengthening public health laboratories, using information technology, and developing human resources for surveillance and response at the district, state, and national levels. IDSP collects surveillance data on various diseases through syndromic, presumptive, and confirmed case reporting. Data flows from the district to state and national levels to allow for analysis and coordinated response.
Introduction to the Integrated Disease Surveillance Project by Dr. Sandeep Das, highlighting the role of AIIMS.
Definition of surveillance in epidemiology; systematic collection and dissemination of data.
Key questions answered by surveillance: disease demographics, incidence, origins, timelines, causes, and required actions.
Timely actions through effective surveillance can prevent potential cases in outbreak scenarios.
Key components of surveillance systems: detection, data collection, analysis, feedback, and responses.
Overview of historical health programs in India and identification of gaps in integration and data usage.
Introduction to NSPCD launched in 1997-98, covering 101 districts, focusing on outbreak reporting.
IDSP: decentralized, state-based surveillance program initiated in 2004, funded by the World Bank.
Details on IDSP's rollout across various states by phases from 2004 to 2007.
Goals of IDSP including establishing a decentralized system and integrating existing surveillance efforts.
List of diseases monitored through regular surveillance, including communicable and non-communicable diseases.
Categories of surveillance: sentinel, regular periodic surveys, and monitoring various health conditions.
Key components integral to IDSP's approach: decentralization, IT use, lab strengthening, and workforce development.
Definitions of different surveillance classifications: syndromic, presumptive, and confirmed.
Who conducts syndromic surveillance and the diseases categorized under this method.
Process of presumptive surveillance conducted by medical officers, including laboratory confirmation.
Overview of reporting forms for health workers concerning suspect, probable, and lab-confirmed cases.
Levels of laboratory responsibility and requirements for reporting cases at various lab types.
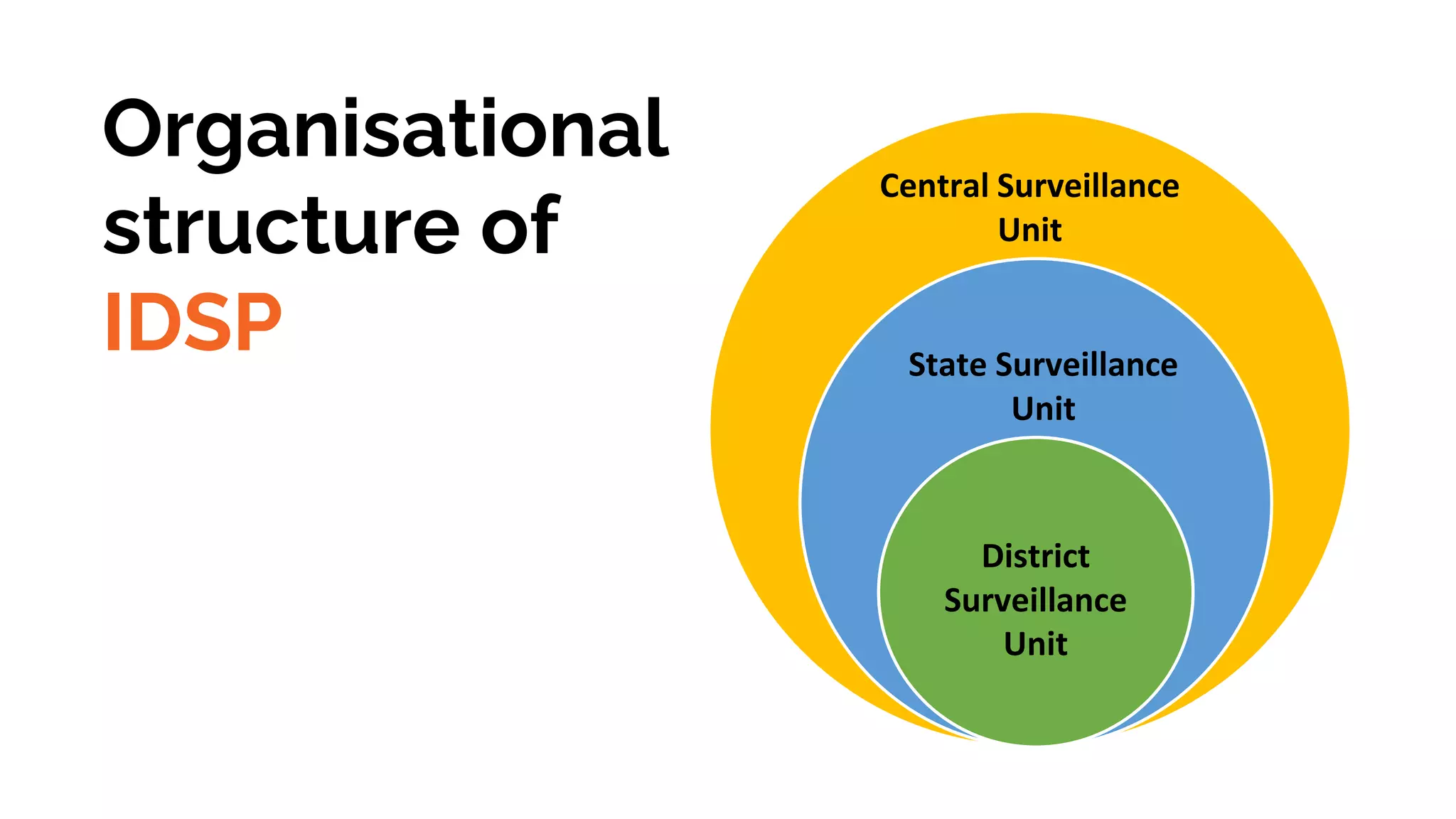
Hierarchical structure of IDSP with Central, State, and District Surveillance Units.
Responsibilities of the National Surveillance Unit in planning, monitoring, and coordinating surveillance activities.
Roles and responsibilities of the State Surveillance Unit including data analysis and rapid response coordination.
Duties of the District Surveillance Unit in data collection, project monitoring, and training coordination.
Comparison of public health sector roles in rural versus urban areas, including different health facilities.
Detailed flow of information relating to weekly surveillance activities from district to central units.
Key performance indicators for evaluating the timeliness and adequacy of surveillance reporting and responses.
Networking relationships of the Central Surveillance Unit with various health programs and organizations.
Different levels of surveillance triggers to respond to outbreaks, specifying local, regional, and state-level actions.
Conditions identifying potential outbreaks including clustering of cases, unusual case increases, and more.
Introduction to IHIP, a web-based system for real-time data reporting and health management.
Goals and objectives of the SHOC for managing disease outbreaks and enhancing response mechanisms.



































































