Obsessive Compulsive Disorder
It’s normal, on occasion, to go back and double-check
that the oven is unplugged or your car is locked.
But if you suffer from obsessive-compulsive disorder
(OCD), obsessive thoughts and compulsive behaviours
become so excessive they interfere with your daily life.
No matter what you do, you can’t seem to shake them.
3.
What is obsessive-compulsive
disorder(OCD)?
Obsessive-compulsive disorder (OCD) is an anxiety disorder
characterized by uncontrollable, unwanted thoughts and repetitive,
ritualized behaviors you feel compelled to perform. If you have
OCD, you probably recognize that your obsessive thoughts and
compulsive behaviors are irrational—but even so, you feel unable to
resist them and break free.
Like a needle getting stuck on an old record, OCD causes the brain
to get stuck on a particular thought or urge. For example, you may
check the stove 20 times to make sure it’s really turned off, or wash
your hands until they’re scrubbed raw.
4.
OTHER DEFINITIONS
Obsessive-compulsivedisorder(OCD) is an anxiety disorder in
which people have recurring, unwanted thoughts, ideas or
sensations (obsessions) that make them feel driven to do something
repetitively (compulsions). (APA,
2008)
Obsessive-compulsive disorder (OCD) features a pattern of
unreasonable thoughts and fears (obsessions) that lead you to do
repetitive behaviors (compulsions). (MCS, 2012)
5.
Obsessions
Obsessions arethoughts, images or impulses that occur over and over again and
feel outside of the person’s control. Individuals with OCD do not want to have these
thoughts and find them disturbing. (Bloch, Landeros-Weisenberger, Sen, et al., 2008).
In most cases, people with OCD realize that these thoughts don’t make any sense.
Obsessions are typically accompanied by intense and uncomfortable feelings
such as fear, disgust, doubt, or a feeling that things have to be done in a way that is
“just right.”
In the context of OCD, obsessions are time consuming and get in the way of
important activities the person values.
SIMPLY PUT---
Obsessions are involuntary thoughts, images, or impulses that occur over and over
again in your mind. You don’t want to have these ideas, but you can’t stop them.
Unfortunately, these obsessive thoughts are often disturbing and distracting
6.
COMPULSIONS
Compulsions arethe second part of obsessive compulsive disorder.
These are repetitive behaviors or thoughts that a person uses with the intention of
neutralizing, counteracting, or making their obsessions go away.
People with OCD realize this is only a temporary solution but without a better way to cope
they rely on the compulsion as a temporary escape.
Compulsions can also include avoiding situations that trigger obsessions. Compulsions are
time consuming and get in the way of important activities the person values.
Simply put-
Compulsions are behaviors or rituals that you feel driven to act out again and again.
Usually, compulsions are performed in an attempt to make obsessions go away.
For example, if you’re afraid of contamination, you might develop elaborate cleaning
rituals.
However, the relief never lasts. In fact, the obsessive thoughts usually come back stronger.
And the compulsive rituals and behaviors often end up causing anxiety themselves as they
become more demanding and time-consuming. This is the vicious cycle of OCD.
7.
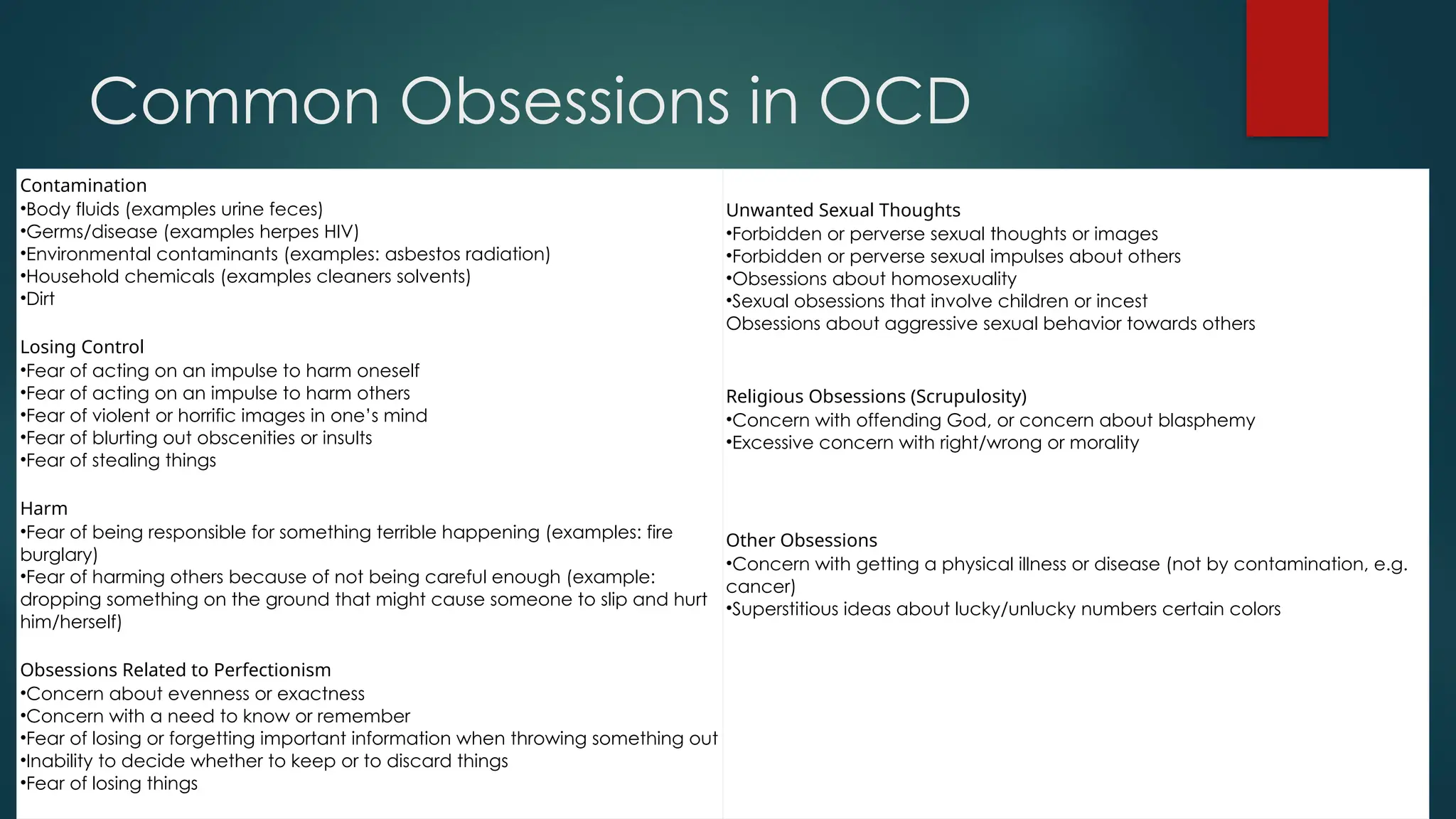
Common Obsessions inOCD
Contamination
•Body fluids (examples urine feces)
•Germs/disease (examples herpes HIV)
•Environmental contaminants (examples: asbestos radiation)
•Household chemicals (examples cleaners solvents)
•Dirt
Losing Control
•Fear of acting on an impulse to harm oneself
•Fear of acting on an impulse to harm others
•Fear of violent or horrific images in one’s mind
•Fear of blurting out obscenities or insults
•Fear of stealing things
Harm
•Fear of being responsible for something terrible happening (examples: fire
burglary)
•Fear of harming others because of not being careful enough (example:
dropping something on the ground that might cause someone to slip and hurt
him/herself)
Obsessions Related to Perfectionism
•Concern about evenness or exactness
•Concern with a need to know or remember
•Fear of losing or forgetting important information when throwing something out
•Inability to decide whether to keep or to discard things
•Fear of losing things
Unwanted Sexual Thoughts
•Forbidden or perverse sexual thoughts or images
•Forbidden or perverse sexual impulses about others
•Obsessions about homosexuality
•Sexual obsessions that involve children or incest
Obsessions about aggressive sexual behavior towards others
Religious Obsessions (Scrupulosity)
•Concern with offending God, or concern about blasphemy
•Excessive concern with right/wrong or morality
Other Obsessions
•Concern with getting a physical illness or disease (not by contamination, e.g.
cancer)
•Superstitious ideas about lucky/unlucky numbers certain colors
8.
Common Compulsions inOCD
Washing and Cleaning
•Washing hands excessively or in a certain way
•Excessive showering, bathing, tooth-brushing, grooming ,or
toilet routines
•Cleaning household items or other objects excessively
•Doing other things to prevent or remove contact with
contaminants
Checking
•Checking that you did not/will not harm others
•Checking that you did not/will not harm yourself
•Checking that nothing terrible happened
•Checking that you did not make a mistake
•Checking some parts of your physical condition or body
Repeating
•Rereading or rewriting
•Repeating routine activities (examples: going in or out
doors, getting up or down from chairs)
•Repeating body movements (example: tapping, touching,
blinking)
•Repeating activities in “multiples” (examples: doing a task
three times because three is a “good,” “right,” “safe”
number)
Mental Compulsions
•Mental review of events to prevent harm (to oneself others,
to prevent terrible consequences)
•Praying to prevent harm (to oneself others, to prevent
terrible consequences)
•Counting while performing a task to end on a “good,”
“right,” or “safe” number
•“Cancelling” or “Undoing” (example: replacing a “bad”
word with a “good” word to cancel it out)
Other Compulsions
•Putting things in order or arranging things until it “feels right”
•Telling asking or confessing to get reassurance
•Avoiding situations that might trigger
9.
Obsessive thoughts
•Common obsessive thoughts in OCD include:
• Fear of being contaminated by germs or dirt or contaminating others
• Fear of losing control and harming yourself or others
• Intrusive sexually explicit or violent thoughts and images
• Excessive focus on religious or moral ideas
• Fear of losing or not having things you might need
• Order and symmetry: the idea that everything must line up “just right”
Superstitions; excessive attention to something considered lucky or unlucky
Compulsive behaviors
• Common compulsive behaviors in OCD include:
• Excessive double-checking of things, such as locks, appliances, and switches
• Repeatedly checking in on loved ones to make sure they’re safe
• Counting, tapping, repeating certain words, or doing other senseless things to reduce anxiety
• Spending a lot of time washing or cleaning
• Ordering or arranging things “just so”
• Praying excessively or engaging in rituals triggered by religious fear
• Accumulating “junk” such as old newspapers or empty food containers
11.
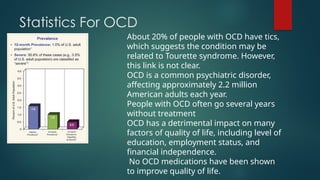
Statistics For OCD
About20% of people with OCD have tics,
which suggests the condition may be
related to Tourette syndrome. However,
this link is not clear.
OCD is a common psychiatric disorder,
affecting approximately 2.2 million
American adults each year.
People with OCD often go several years
without treatment
OCD has a detrimental impact on many
factors of quality of life, including level of
education, employment status, and
financial independence.
No OCD medications have been shown
to improve quality of life.
12.
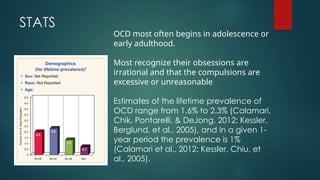
STATS
OCD most oftenbegins in adolescence or
early adulthood.
Most recognize their obsessions are
irrational and that the compulsions are
excessive or unreasonable
Estimates of the lifetime prevalence of
OCD range from 1.6% to 2.3% (Calamari,
Chik, Pontarelli, & DeJong, 2012; Kessler,
Berglund, et al., 2005), and in a given 1-
year period the prevalence is 1%
(Calamari et al., 2012; Kessler, Chiu, et
al., 2005).
13.
DSM IV TRCriteria
A. Either obsessions or compulsions:
Obsessions as defined by (1), (2), (3), and (4):
(1) recurrent and persistent thoughts, impulses, or images that are experienced at
some time during the disturbance, as intrusive and inappropriate and that cause
marked anxiety or distress
(2) the thoughts, impulses, or images are not simply excessive worries about real-life
problems
(3) the person attempts to ignore or suppress such thoughts, impulses, or images, or
to neutralize them with some other thought or action
(4) the person recognizes that the obsessional thoughts, impulses, or images are a
product of his or her own mind (not imposed from without as in thought insertion)
14.
Compulsions asdefined by (1) and (2):
(1) repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting,
repeating words silently) that the person feels driven to perform in response to an obsession, or
according to rules that must be applied rigidly
(2) the behaviors or mental acts are aimed at preventing or reducing distress or preventing some
dreaded event or situation; however, these behaviors or mental acts either are not connected in a
realistic way with what they are designed to neutralize or prevent or are clearly excessive
B. At some point during the course of the disorder, the person has recognized that the obsessions or
compulsions are excessive or unreasonable. Note: This does not apply to children
C. The obsessions or compulsions cause marked distress, are time consuming (take more than 1 hour a
day), or significantly interfere with the person’s normal routine, occupational (or academic) functioning,
or usual social activities or relationships.
D. If another Axis I disorder is present, the content of the obsessions or compulsions is not restricted to
it (e.g., preoccupation with food in the presence of an Eating Disorder; hair pulling in the presence of
Trichotillomania; concern with appearance in the presence of Body Dysmorphic Disorder; preoccupation
with drugs in the presence of a Substance Use Disorder; preoccupation with having a serious illness in
the presence of Hypochondriasis; preoccupation with sexual urges or fantasies in the presence of a
Paraphilia; or guilty ruminations in the presence of Major Depressive Disorder).
E. The disturbance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a
medication) or a general medical condition.
Specify if:
With poor insight: if, for most of the time during the current episode, the person does not recognize
that the obsessions and compulsions are excessive or unreasonable.
15.
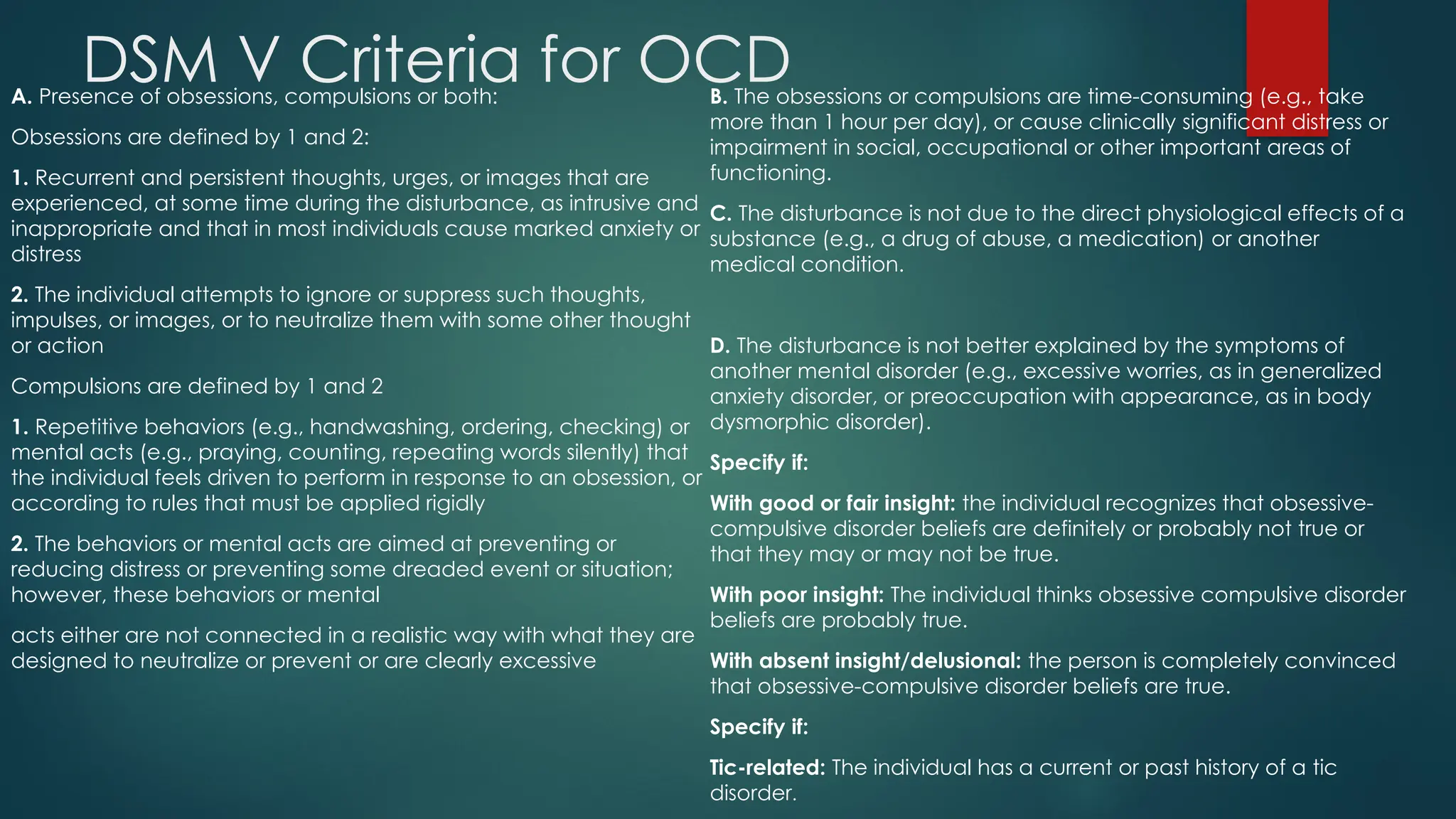
DSM V Criteriafor OCD
A. Presence of obsessions, compulsions or both:
Obsessions are defined by 1 and 2:
1. Recurrent and persistent thoughts, urges, or images that are
experienced, at some time during the disturbance, as intrusive and
inappropriate and that in most individuals cause marked anxiety or
distress
2. The individual attempts to ignore or suppress such thoughts,
impulses, or images, or to neutralize them with some other thought
or action
Compulsions are defined by 1 and 2
1. Repetitive behaviors (e.g., handwashing, ordering, checking) or
mental acts (e.g., praying, counting, repeating words silently) that
the individual feels driven to perform in response to an obsession, or
according to rules that must be applied rigidly
2. The behaviors or mental acts are aimed at preventing or
reducing distress or preventing some dreaded event or situation;
however, these behaviors or mental
acts either are not connected in a realistic way with what they are
designed to neutralize or prevent or are clearly excessive
B. The obsessions or compulsions are time-consuming (e.g., take
more than 1 hour per day), or cause clinically significant distress or
impairment in social, occupational or other important areas of
functioning.
C. The disturbance is not due to the direct physiological effects of a
substance (e.g., a drug of abuse, a medication) or another
medical condition.
D. The disturbance is not better explained by the symptoms of
another mental disorder (e.g., excessive worries, as in generalized
anxiety disorder, or preoccupation with appearance, as in body
dysmorphic disorder).
Specify if:
With good or fair insight: the individual recognizes that obsessive-
compulsive disorder beliefs are definitely or probably not true or
that they may or may not be true.
With poor insight: The individual thinks obsessive compulsive disorder
beliefs are probably true.
With absent insight/delusional: the person is completely convinced
that obsessive-compulsive disorder beliefs are true.
Specify if:
Tic-related: The individual has a current or past history of a tic
disorder.
16.
Risk Factors// CAUSES
OCD is a common disorder that affects adults, adolescents, and children all over the world.
Most people are diagnosed by about age 19, typically with an earlier age of onset in boys
than in girls, but onset after age 35 does happen.
The causes of OCD are unknown, but risk factors include:
Biology. OCD may be a result of changes in your body's own natural chemistry or brain
functions.
Genetics. OCD may have a genetic component, but specific genes have yet to be
identified.
Environment. Some environmental factors such as infections are suggested as a trigger for
OCD, but more research is needed.
17.
Genetics
Someresearch points to the likelihood that OCD sufferers will have a family
member with the problem or with one of the other ‘OCD –Spectrum’ of
disorders.
One American study suggested that up to 30% of teenagers with OCD had a
member of the immediate family with the problem or with obsessive symptoms.
Other studies tend to suggest that if a sufferer’s OCD began in adulthood there
is less chance of this person’s offspring contracting it than if the problem was
contracted in childhood, specifically if the latter is the type of OCD that tends
to start in childhood (if there are different types).
Twin and family studies have shown that people with first-degree relatives (such
as a parent, sibling, or child) who have OCD are at a higher risk for developing
OCD themselves. The risk is higher if the first-degree relative developed OCD as
a child or teen. Ongoing research continues to explore the connection
between genetics and OCD and may help improve OCD diagnosis and
treatment.
18.
BIOLOGY
Brain Structureand Functioning
Imaging studies have shown differences in the frontal cortex and subcortical structures of the
brain in patients with OCD. There appears to be a connection between the OCD symptoms
and abnormalities in certain areas of the brain, but that connection is not clear. Research is
still underway. Understanding the causes will help determine specific, personalized
treatments to treat OCD.
Chemical and brain dysfunction
The chemical messenger, Serotonin seems to be heavily involved. Serotonin is a chemical called
a neurotransmitter that allows nerve cells to communicate with each other by working in the
space between nerve cells, called the synaptic cleft.
According to research, Serotonin is involved with biological processes such as mood,
aggression, sleep, appetite and pain. It also seems that Serotonin is capable of connecting to
nerve cells in the brain in many different ways and so can cause many different responses. It
is not even fully established if it is all or part of the Serotonin chemical or another chemical
entirely acting on it; or a malfunction in one or more of the receptors in the brain that
Serotonin attaches to that causes the OCD problems
19.
Environment
People whohave experienced abuse (physical or sexual) in
childhood or other trauma are at an increased risk for developing
OCD.
In some cases, children may develop OCD or OCD symptoms
following a streptococcal infection—this is called Pediatric
Autoimmune Neuropsychiatric Disorders Associated with
Streptococcal Infections (PANDAS).
20.
TREATMENT
OCD istypically treated with medication, psychotherapy or a combination of the two.
Although most patients with OCD respond to treatment, some patients continue to
experience symptoms.
Sometimes people with OCD also have other mental disorders, such as anxiety,
depression, and body dysmorphic disorder, a disorder in which someone mistakenly
believes that a part of their body is abnormal. It is important to consider these other
disorders when making decisions about treatment.
21.
Medication
Serotonin reuptakeinhibitors (SRIs) and selective serotonin reuptake
inhibitors (SSRIs) are used to help reduce OCD symptoms. Examples
of medications that have been proven effective in both adults and
children with OCD include clomipramine , which is a member of an
older class of “tricyclic” antidepressants, and several newer
“selective serotonin reuptake inhibitors” (SSRIs), including:
fluoxetine
fluvoxamine
sertraline
22.
Psychotherapy
Psychotherapy canbe an effective treatment for adults and children
with OCD. Research shows that certain types of psychotherapy,
including cognitive behavior therapy (CBT) and other related therapies
(e.g., habit reversal training) can be as effective as medication for
many individuals.
Research also shows that a type of CBT called Exposure and Response
Prevention (EX/RP) is effective in reducing compulsive behaviors in
OCD, even in people who did not respond well to SRI medication. For
many patients EX/RP is the add-on treatment of choice when SRIs or
SSRIs medication does not effectively treat OCD symptoms.