![Infectious diseases Pharmacotherapy
Lesson 2
Upper respiratory tract infections[URTIs]
By: Tsegaye Melaku [MSc]
tsegayemlk@yahoo.com or tsegaye.melaku@ju.edu.etJuly, 2018 +251913765609+251913765609
Upper respiratory tract infections[URTIs]](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-1-2048.jpg)


![URTIs: comprehensive term for upper airway infections
[otitis media, sinusitis, pharyngitis, laryngitis, common cold
& other].
3 most common: of bacteria cause3 most common: of bacteria cause
Otitis media.
Pharyngitis.
Sinusitis.
Less common: laryngitis, rhinitis, and epiglottitis.
4](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-4-2048.jpg)













![ Acute onset of ear pain.
Irritability & tugging on the ear clue for Dx in young children.
Otitis media with effusion
– Fluid in the middle ear with no S & Sxsno S & Sxs of acute ear
infection [pain & bulging eardrum].
18](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-18-2048.jpg)



![ General
Acute onset: runny nose, nasal congestion, or cough
Signs and Symptoms
Ear pain [severe] (>75% of patients)
22
Irritable, tug on the involved ear,& have difficulty sleeping
Fever (<25% of patients), more often in younger children](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-22-2048.jpg)
![Discolored (gray), thickened, bulging eardrum
On pneumatic otoscopy/tympanometry [immobile
eardrum]; ~~50% cases…bilateral
Draining middle ear fluid occurs [<3%]Draining middle ear fluid occurs [<3%]
Laboratory tests
Gm stain, culture, and sensitivities
Adapted from Hendley JO. Clinical practice: Otitis media. N Engl J Med
2002;347(15):1169–1174.
23](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-23-2048.jpg)







![ 1st Differentiate AOM from OME or COM the latter 2 do not
benefit from abx.
– Tympanostomy tube placement with or without
adenoidectomy
2nd address pain [oral analgesics].
3rd Consider if a brief observation period is warranted.
– Majority of uncomplicated cases resolve spontaneously.
31](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-31-2048.jpg)
![ Watchful waiting and “safety-net” antibiotic prescriptions!!
APAP or
NSAID (ibuprofen): early to relieve pain.
– Avoided in children <6 months [increased toxicity– Avoided in children <6 months [increased toxicity
concerns]
Ear-drops with a local anesthetic
Don’t use decongestants or antihistamines routinely
– Minimal benefit and increased side effects.
33](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-33-2048.jpg)



![ High-dose amoxicillin: overcome resistance
[80 to 90 mg/kg/day] vs [40–45 mg/kg/day]
» Results in higher middle ear fluid concentrations
Change Rx: if complications symptoms unresolved within 3
days.
37](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-37-2048.jpg)
![ High dose amoxicillin-clavulanate:
(Amox. 90 mg/kg/day/Clav. 6.4 mg/kg/day) into 2
doses
Considered for
– Who received amoxicillin within 30 days,– Who received amoxicillin within 30 days,
– Concurrent purulent conjunctivitis,
– Hx of recurrent AOM unresponsive to amoxicillin
– Suspected ß-lactamase producing organisms.
– Moderate to severe illness ( T˚>39°C [102°F] and/or
severe otalgia),
38](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-38-2048.jpg)
![ 2nd line agents:
2nd-gen. cephalosporins
Cefuroxime, cefdinir, cefpodoxime,
Ceftriaxone.
[ß-lactamase stable, expensive, increased incidence of side [ß-lactamase stable, expensive, increased incidence of side
effects].
Trimethoprim-sulfamethoxazole and macrolides
Have limited efficacy against S. pneumoniae and H.
influenzae
Not DOC
39DRSP: drug-resistant S. pneumoniae](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-39-2048.jpg)
![ Ceftriaxone :
Achieve MIC for >40% of the dosing interval at middle ear
50 mg/kg/day IM/IV stat have been used.
– But, daily doses for 3 days are recommended to optimize
clinical outcomes.clinical outcomes.
Reserved for:
– Severe and unresponsive infections or
– Unable to take PO (V, D, or non-adherence].
40](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-40-2048.jpg)
![ Penicillin allergic patients
Non-type I [non- IgE] hypersensitivity
– Cefdinir, cefpodoxime, or cefuroxime
Type I (anaphylactic) [IgE]Type I (anaphylactic) [IgE]
– Macrolide (azithromycin or clarithromycin)
Clindamycin:
– If penicillin allergy + documented S. pneumoniae
– To cover PRSP.
41](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-41-2048.jpg)


![ Defined: at least 3 episodes in ½ yr or at least 4 episodes in 1yr.
Concern in < 3 yrs children;
[at high risk for hearing loss and language and learning
disabilities].
Do not use prophylaxis.Do not use prophylaxis.
Use of tympanostomy tubes (TUse of tympanostomy tubes (T--tubes): effective its preventiontubes): effective its prevention
Current insight: Oral fluoroquinolones ???
44](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-44-2048.jpg)












![ Mxm not well defined
If alteration in host immunity (a breach in the pharyngeal mucosa)
If disruption in mucosal integrity
Asymptomatic pharyngeal carriers or colonization by
GABHS InfectionInfection
Pathogenic factors associated with the organism [pyrogenic
toxins, hemolysins, streptokinase, and proteinase] itself play
a role.
57](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-57-2048.jpg)











![ The pink membranes lining the sinuses make mucus
Which is cleared out of the sinus cavities drains into the
nasal passage.
Both airflow & mucus ends up in a part of throat [nasopharynx] Both airflow & mucus ends up in a part of throat [nasopharynx]
Air is then breathed into the windpipe and lungs, while the
mucus is swallowed
70](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-70-2048.jpg)
![ Other structures associated with the nasal and sinus tract:
Tear duct (nasolacrimal duct): drains tears from the inside corner
of the eye into the nasal cavity
Eustachian tube: responsible for clearing air pressure in the ears; it
opens into the back of the sidewall of the nasopharynx.
Adenoids: collection of tonsil-like tissue [at top of the nasopharynx]
71](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-71-2048.jpg)




![ Inflammation and/or infection of the para-nasal sinuses
Aka rhinosinusitis [involves contiguous nasal mucosa]
Occurs in nearly all viral URIsall viral URIs
76
Sinusitis
Acute
Chronic
Symptoms persist for up to 4 wks
Lasts for more than 12 weeks.](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-76-2048.jpg)

![ Mainly respiratory viruses
Can be triggered by allergies or environmental irritantsallergies or environmental irritants..
Complicated rhinosinusitis [2° bacterial infection]: 22 --13%.13%.
Viral: Usually improves in 5-7 days
Bacterial: if severe & symptoms > 10 days or worsens after 5-7
daysdays
Most common
• Streptococcus pneumoniae
• Haemophilus influenzae
• Moraxella catarrhalis
Less Frequent
• Streptococcus pyogenes
• Staphylococcus aureus
• Gram-negative bacilli
• Anaerobes
78](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-78-2048.jpg)










![ Goals of therapy
Relieve symptoms
Promote sinus drainage/achieve & maintain patency of the ostia
Use antibiotics when appropriate[minimize resistance] Use antibiotics when appropriate[minimize resistance]
Prevent development of chronic disease or complications
89](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-89-2048.jpg)



![ Antihistamines
Should not be used for acute bacterial sinusitis
– Have anticholinergic effects
2nd-generation : have a role in chronic sinusitis,
– Because frequently accompanied by concomitant allergic rhinitis.
Glucocorticoids [intranasal]
Decrease inflammation causing headache, nasal congestion, and
facial pain.
But, limited data to support
93](https://image.slidesharecdn.com/upperrespiratorytractinfections-180907144819/75/Pharmacotherapy-of-Upper-respiratory-tract-infections-93-2048.jpg)














This document provides information on upper respiratory tract infections (URTIs) with a focus on otitis media. It discusses the common bacterial causes of otitis media, including Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. It also outlines the signs and symptoms of acute otitis media, including ear pain, fever, and bulging of the eardrum. The document recommends amoxicillin as the first-line treatment and discusses alternative antibiotic options if needed. It emphasizes the importance of differentiating between acute otitis media and otitis media with effusion to determine appropriate treatment.
This section introduces URTIs (upper respiratory tract infections), focusing on antimicrobial initiation concerns and clinical management.
Defines URTIs, common bacterial causes, including otitis media, pharyngitis, and sinusitis, highlights viral origins and concerns about antibiotic resistance.
Focuses on otitis media, types (acute, with effusion), diagnosis, and prevalence. Emphasizes the importance of antibiotic use and management.
Discusses otitis media's epidemiology, common pathogens, and risk factors contributing to antibiotic resistance.
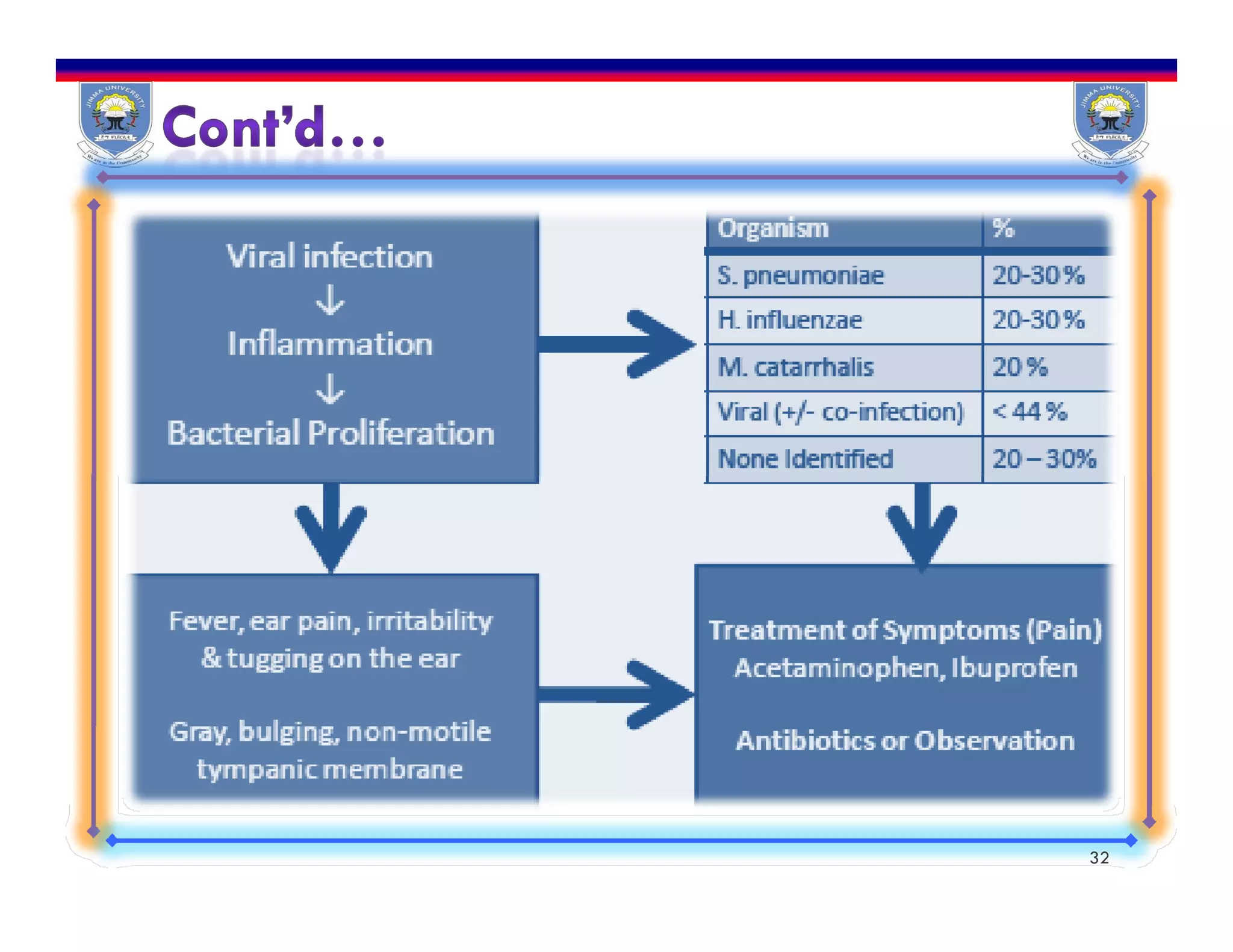
Examines the pathophysiology and progression of AOM, outlining how URTIs lead to infections affecting the middle ear.
Outlines the criteria for diagnosing AOM, focusing on symptoms and physical findings necessary for accurate evaluation.
Identifies significant symptoms in patients with AOM, including clinical signs of ear infection for diagnosis.
Discusses potential complications from AOM like meningitis and auditory sequelae, highlighting risks and the need for treatment.
Outlines treatment goals, emphasizes prudent antibiotic use, and strategies like watchful waiting and pain management.
Details antibiotic therapy guidelines, including first-line treatments and considerations for antibiotic-resistant infections.
Describes procedures like tympanocentesis and antibiotic regimens, providing dosages and special considerations.
Introduces pharyngitis, outlining clinical presentation, evaluation, and risk factors associated with streptococcal infections.
Highlights potential complications of untreated pharyngitis and presents the common viral and bacterial pathogens involved.
Describes clinical features of pharyngitis, apparent during physical examinations, and includes laboratory testing options.
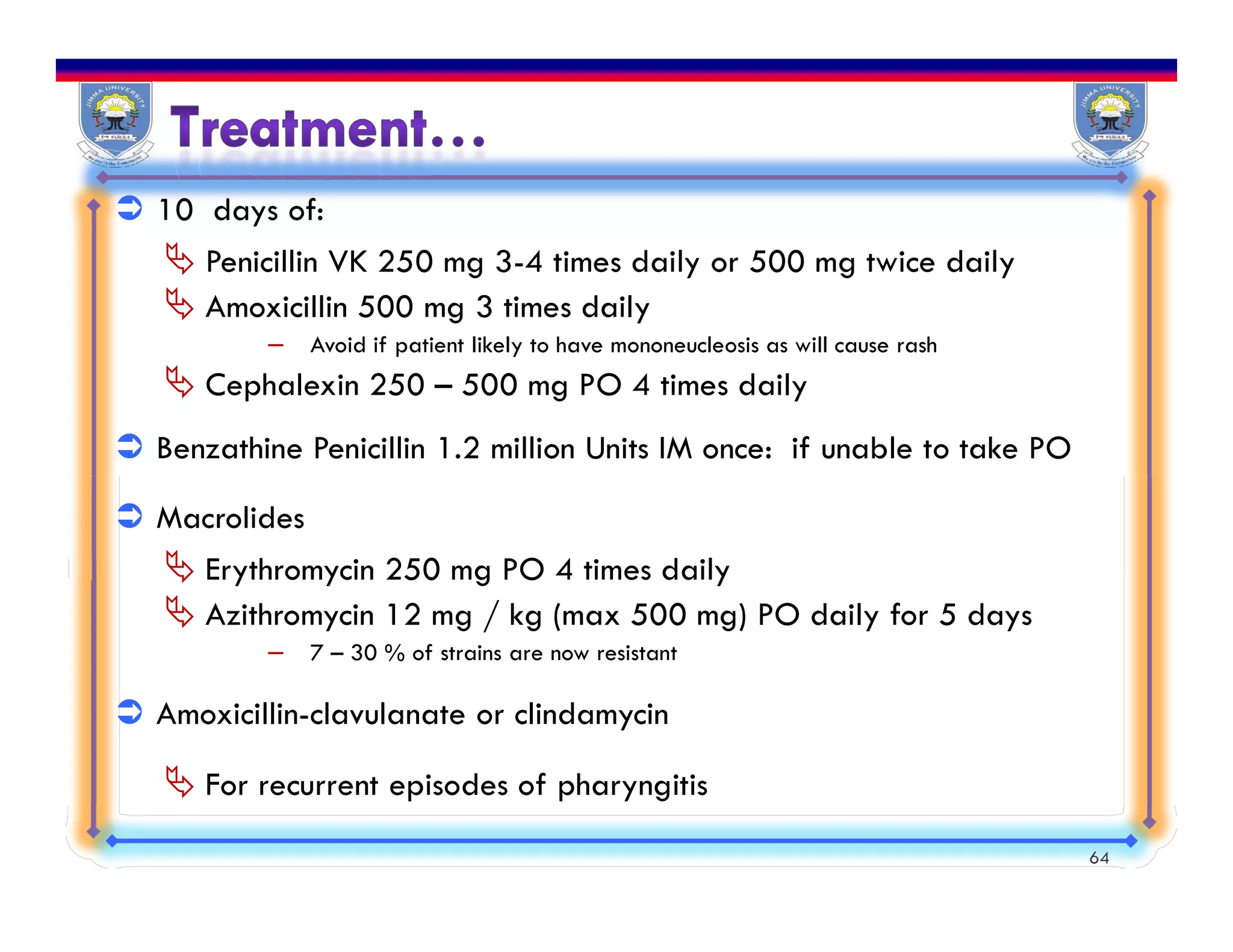
Focuses on treatment goals, requires eradication of GABHS, symptom management, and appropriate antibiotic use.
Presents common antibiotic options with adult and pediatric dosages for effective treatment of infections.Introduces sinusitis, describing its symptoms, the involved anatomical structures, and overall prevalence.
Discusses incidence rates of sinusitis, its costs, and triggers like allergies and environmental factors.
Differentiates chronic and acute sinusitis, listing symptoms, necessary laboratory tests, and appropriate treatments.
Details the recommended antibiotic treatments for sinusitis, including alternatives for patients with penicillin allergies.
Summarizes key clinical presentations, diagnostic aids, and defines appropriate management for various URTIs.






















































































