This document provides information on sample size estimation. It discusses the importance of sample size estimation and how the objective of the study determines whether sample size needs to be estimated. It provides examples of sample size calculation for pilot studies, estimation studies, and hypothesis testing studies. Formulas are presented for estimating parameters like prevalence, sensitivity and specificity as well as for testing differences between groups. The document emphasizes setting significance levels and power appropriately depending on the goals of the study.
Explains the importance of sample size estimation in studies to yield reliable results.
Discusses reasons for sufficient sample size: too small is a waste, too large wastes resources, can be unethical.
Differentiates between hypothesis generation (no sample size needed) and confirmation (sample size estimation required).
Provides examples of pilot studies with specified sample sizes to generate hypotheses about treatment effects.
Details on determining sample size for hypothesis confirmation focusing on parameter estimation and testing.
Summarizes formulas related to estimating proportions and means, emphasizing 95% confidence intervals.
Introduces formulas and examples for testing differences in proportions and means with sample size requirements. Illustrates examples for estimating prevalence and sensitivity/specificity with confidence intervals and sample sizes.
Analyzes study design examples focusing on hypothesis testing using sample size derived from sensitivity estimations.
Explains sample size estimation for means specifying population parameters and expected margins of error.
Explains sample size determination for trials, contrasting statistical and clinical significance with examples.
Discusses Type I (α) and Type II (β) errors, their impact, and common thresholds used in trials.
Details calculations for sample size based on Chi-square tests including correction factors.
Describes canonical examples for sample size determination in testing treatment efficacy during clinical trials.
Details on planning sample sizes for differences in means, including drop-out considerations and power calculations.
Discusses testing the significance of proportions and means, emphasizing correlation in studies.
Cautions on the assumptions made in sample size calculations and methods for estimating sizes.
List of literature and references that provide statistical methodologies related to sample size estimation.
Sample Size Estimation
•Why ?
- n is large enough to provide a reliable answer to the
question
- too small n
a waste of time
- too many n
a waste of money & other resources
May be unethical
e.g., delayed beneficial therapy
placebo
3.
• Study Objective:
-Hypothesis generating (Pilot study)
No sample size estimation
- Hypothesis confirmation
Sample size estimation
- n is usually determined by the primary objective
of the study
- method of calculating n should be given in the
proposal, together with the assumptions made
in the calculation
4.
Pilot study
Example: (Mar23,1999, #1515)
This study for n=20 eligible burn patients
will generate hypothesis about the predictive
values of various patient characteristics
for predicting number of days to return to
work.
5.
Pilot study (cont’d)
Example:(Oct 27, 1998, #1465)
This is a pilot study providing preliminary
descriptive statistics that will be used to
design a larger, adequately powered study.
N=24 normal healthy volunteers will be
randomized to parallel groups to study the
effect of 4 antidepressant drugs…
6.
Hypothesis confirmation study
Samplesize determination: 2 Objectives
I. Estimation of parameter(s)
Precision (95% CI)
Specify α error
- Estimate prevalence, sensitivity, specificity
- Estimate single mean, single proportion
- etc.
7.
II. Test H0
Statisticalpower (1- β)
Specify α, β error
2.1 Single group
- Test of single proportion, mean
- Test of Pearson’s correlation
- etc.
2.2 Two groups
- Test difference of
- 2 independent proportions, means, survival curves
- 2 dependent proportions, means
- Test equivalence of
- 2 independent proportions, means
- etc.
2.3 > 2 groups
8.
Commonly used formulas:Summary
1)
Estimation
1.1) Estimate single proportion
95% CI of π = p ± d
(π = True pop’n proportion
p = Expected proportion e.g., prevalence
q = 1-p
d = Margin of error in estimating p)
2
zα/2 pq
n =
d2
1.2) Estimate single mean
95% CI of μ =⎯x ± d
(μ = True pop’n mean
⎯x = Expected mean
d = Margin of error in estimating mean)
n = [zα/2 SD / d]2
9.
2)
Test
2.1) Test ofdifference in 2 independent proportions (p1, p2)
p1, p2 = Proportion of … in group 1 and 2
p
= (p1+p2)/2
n/group = [
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
2.2) Test of difference in 2 independent means (Δ)
σ = Common SD of outcome var. in group 1, 2
Δ = Difference in mean b/t 2 groups
n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
2.3) Test of difference in > 2 independent means
]2
10.
2.4) Test ofsignificance of 1 proportion
H0: π = π0
H1: π = π1
n =[
zα p 0 q 0 + z β p1q1
p 0 − p1
2.5) Test of significance of 1 mean
H0: μ = μ0
H1: μ = μ1
Δ = |μ1 - μ0|
σ = SD of outcome var.
n = [
(z α + z β )σ
Δ
]2
]2
11.
2.6) Test ofsignificance of 1 correlation
n
F(Z)
=
=
(Zα/2 + Zβ) 2 + 3
[F(Z0) + F(Z1)]
0.5 ln [(1+ρ)/(1-ρ)]
12.
I. Estimation
1.1 EstimatePrevalence
Example: (Mar 18, 2000, #1688)
This is a cross-sectional study of the prevalence
of pulmonary hypertension (PHT) in patients aged
15-70 years with sickle cell disease.
The primary endpoint is PHT diagnosis based
on observed pulmonary pressure by droppler
echocardiogram.
A sample of n = 140 will provide 95% CI for true
prevalence rate of PHT of 0.10 ± 0.05.
13.
95% CI fortrue prevalence (π) = 0.10 ± 0.05
(1- α)100%
″
= p ± d
= p ± zα/2√pq/n
d = zα/2√pq/n
solve for n
2
zα/2 pq
n =
2
d
where
p = estimated prevalence = 0.1
q = 1-p
= 0.9
d = allowable error in estimating prevalence
(margin of error)
= 0.05
α = probability of type I error
= 0.05 (2-sided), z 0.025 = 1.96
1.96 2 (0.1)(0.9)
n =
= 138.3 = 139
2
0.05
14.
How big isd ?
1. Absolute d
2. Relative d: d ≤ 20% of prevalence(p)
p
d
95% CI
n
0.80
0.05*p = 0.04
0.05
0.10*p = 0.08
0.10
0.15*p = 0.12
0.15
0.20*p = 0.16
0.20
0.76, 0.84
0.75, 0.85
0.72, 0.88
0.70, 0.90
0.68, 0.92
0.65, 0.95
0.64, 0.96
0.60, 1.00
384
246
96
62
43
28
24
16
2
zα/2 pq
n =
2
d
pq
d (error)
α
n
15.
I. Estimation (cont’d)
1.2Estimate Sensitivity, Specificity
Example:
- 95% CI for Sensitivity = 85% ± 5%
- 95% CI for Specificity = 90% ± 5%
nDi
=?
nNon-Di = ?
Gold standard
+
Test +
a
b
c
d
a+c
b+d
Sensitivity = a / (a+c)
Specificity = d / (b+d)
Sensitivity
Specificity
p±d
85 ± 5
90 ± 5
95% CI
(80, 90)
(85, 95)
n
= 196
nDi
nNon-Di = 139
16.
Ex.
Title: Diagnosis ofBenign Paraxysmal Positional Vertigo (BPPV)
by Side-lying test as an alternative to the Dix-Hallpike test
Investigator: Dr. Saowaros Asawavichianginda
Design:
Diagnostic study
Subjects:
Dizzy patients, aged 18-80 yrs, onset < 2 wks
Dizzy pts.
1. Dix-Hallpike test
2. Side-lying test
BPPV
No BPPV
17.
Sample size: Basedon 95% CI of true sensitivity (Sn) = 0.9 ± 0.1
2
zα/2 pq
n =
2
d
where
p
q
d
α
=
=
=
=
expected sensitivity = 0.9
1-p = 0.1
allowable error = 0.1
0.05 (2-sided), Z0.025 = 1.96
So, n = 34.56 = No. of patients with BPPV from Dix-Hallpike test
Since prevalence of BPPV among dizzy patients = 40%
Thus, no. of dizzy patients = 34.56 = 86.4 = 87
0.4
Dix-Hallpike test (Gold std)
+ (BPPV)
- (No BPPV)
Side-lying test
+
Sn
-
1 – Sn
35
52
87
18.
1.3 Estimation of1 Mean
การศึกษานี้มีวัตถุประสงคเพื่อประมาณคาเฉลี่ยของ subcarinal angle
ในคนไทยปกติ และจากการศึกษาของ ... ในคนปกติจํานวน 100 รายอายุ ... ป
พบวาคาเฉลี่ยของ subcarinal angle เทากับ 60.8 (SD=11.8)
ถากําหนดให 95% confidence interval (CI) ของคาเฉลี่ยของ
subcarinal angle ในประชากรไทย (μ) มีคาเทากับ 61 ± 2 (SD=13)
จะตองทําการศึกษาในคนไทยปกติจํานวน 163 คนดังรายละเอียดการคํานวณดังนี้
เมื่อ
ดังนั้น
n = [zα/2 SD / d]2
SD = Standard deviation ของ subcarinal angle
= 13
d = Margin of error ในการประมาณคาเฉลี่ย = 2
α = Probability of type I error (2-sided) = 0.05
z0.025 = 1.96
n = [1.96*13/2]2 = 162.31 = 163
19.
II. Test
2.1 Testfor Difference in 2 Independent Proportions
Example: (May 25, 1999, #1549)
This is a randomized (1:1), double-blind,
parallel-group, multi-center trial of drug A (dose1, 2)
in chronic hepatitis C patients aged 18+ years.
The primary efficacy endpoint is sustained viral
response rate after treatment.
N = 141 per group will provide 80% power to detect
an absolute difference in sustained viral response rate
of 11% (7% vs. 18%) at 2-sided α of 0.05.
20.
Clinical significance vs.Statistical significance
N = 141 per group will provide 80% power to detect
an absolute difference in sustained viral response rate
of 11% (7% vs. 18%) at 2-sided α of 0.05.
Clinical (Practical) significance
Statistical significance
21.
Hypotheses
or
or
where
H0
H1
H1
H1
:
:
:
:
π1 - π2
π1- π2
π1 - π2
π1 - π2
=
≠
>
<
0
0 (2-sided)
0 (1-sided, upper tail)
0 (1-sided, lower tail)
π1 = True (population) response rate in group 1
π2 = True (population) response rate in group 2
1-sided, 2-sided test
n (2-sided test)
> n (1-sided test)
2-sided test is conservative
use more often
Decision to use either 1- or 2-sided test should be
made at the design stage, not after looking at the data
22.
α, β (Efficacytrial)
Truth
H0 true
(A=B)
Decision
(from p-value)
Accept H0
Reject H0
No error (1- α)
α
H0 false
(A≠B, Difference)
β
No error (1- β)
Power
α
= Pr (incorrect conclusion of difference
= False positive (FP)
β
=
=
=
=
1-β
)
Pr (incorrect conclusion of equivalence)
False negative (FN)
Pr ( correct conclusion of difference )
True positive (TP)
24.
Truth
H0 true
(Not guilty)
DecisionAccept H0
(Not guilty)
Reject H0
(Guilty)
H0 false
(Guilty)
No error, 1-α
Type II error, β
Type I error, α
No error, 1-β,
Power
α = Probability of wrongly put innocent person into jail
β = Probability of wrongly set the criminal free
1-β = Probability of correctly put criminal into jail
α is more important than β, so usually set β = 4 α
25.
How big isα, β?
1. Type I error (α, test size, significance level)
- To replace a standard drug with a new drug,
type I error is serious,
use small α (0.01, 0.02)
- To add to the body of the published knowledge,
type I error is less serious
use α = 0.05, 0.10
2. Type II error (β)
- Power (1 - β)
- Power is conventionally set at 80% - 90%
- Typically, α is 4 times as serious as β
α = 0.05, β = 0.20 (power = 0.80)
26.
Calculation: n1 =n2 = n
Based on Chi-square test without continuity correction
Zα if 1-sided
n/group = [
where
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
]2
p1 = response rate in group 1 = 0.07
= 0.93
q1 = 1 - p1
p2 = response rate in group 2 = 0.18
q2 = 1 – p2
= 0.82
p
q
= (p1 + p2) / 2
= 1–p
α = 0.05 (2-sided),
1- β = 0.80,
n/group = 141
= 0.125
= 0.875
z0.025 = 1.96
z0.2
= 0.842
27.
n / group
α= 0.05
2-sided 1-sided
p1
p2
Power
7
18
80
90
141
188
111
153
7
20
80
90
108
144
85
117
(p1 – p2)
Power
α
n
28.
Calculation: n1 =n2 = n
Based on Chi-square test with continuity correction
n′ =
n
4
⎤
⎡
4
⎥
⎢1 + 1 +
n p1 - p 2 ⎥
⎢
⎦
⎣
2
141 ⎡
4
=
⎢1 + 1 +
4 ⎢
141 0.18 - 0.07
⎣
= 158.7 ~ 159
⎤
⎥
⎥
⎦
2
29.
Ex:
Title: Efficacy ofpolyethylene plastic wrap for the prevention of
hypothermia during the immediate postnatal period in low
birth weight premature infants
Investigator: Dr. Santi Punnahitananda
Design:
RCT, 2-parallel arms
Subjects: Infants with ≤ 34 gestational wks, birth weight ≤ 1800 gms
Outcome: Infant’s body temperature taken on nursery admission
Infants, ≤ 34 gestational wks, BW ≤ 1800 gms
Randomization
Plastic wrap
No Plastic wrap
Body temp.
Hypothermia
Body temp.
Hypothermia
30.
Sample size estimation:Based on Test of 2 independent proportions
Our unit
hypothermia in low birth weight, premature infants = 55%
(p1 = 0.55)
Assume that plastic wrap would reduce hypothermia to 20%
(p2 = 0.2)
n/group = [
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
]
2
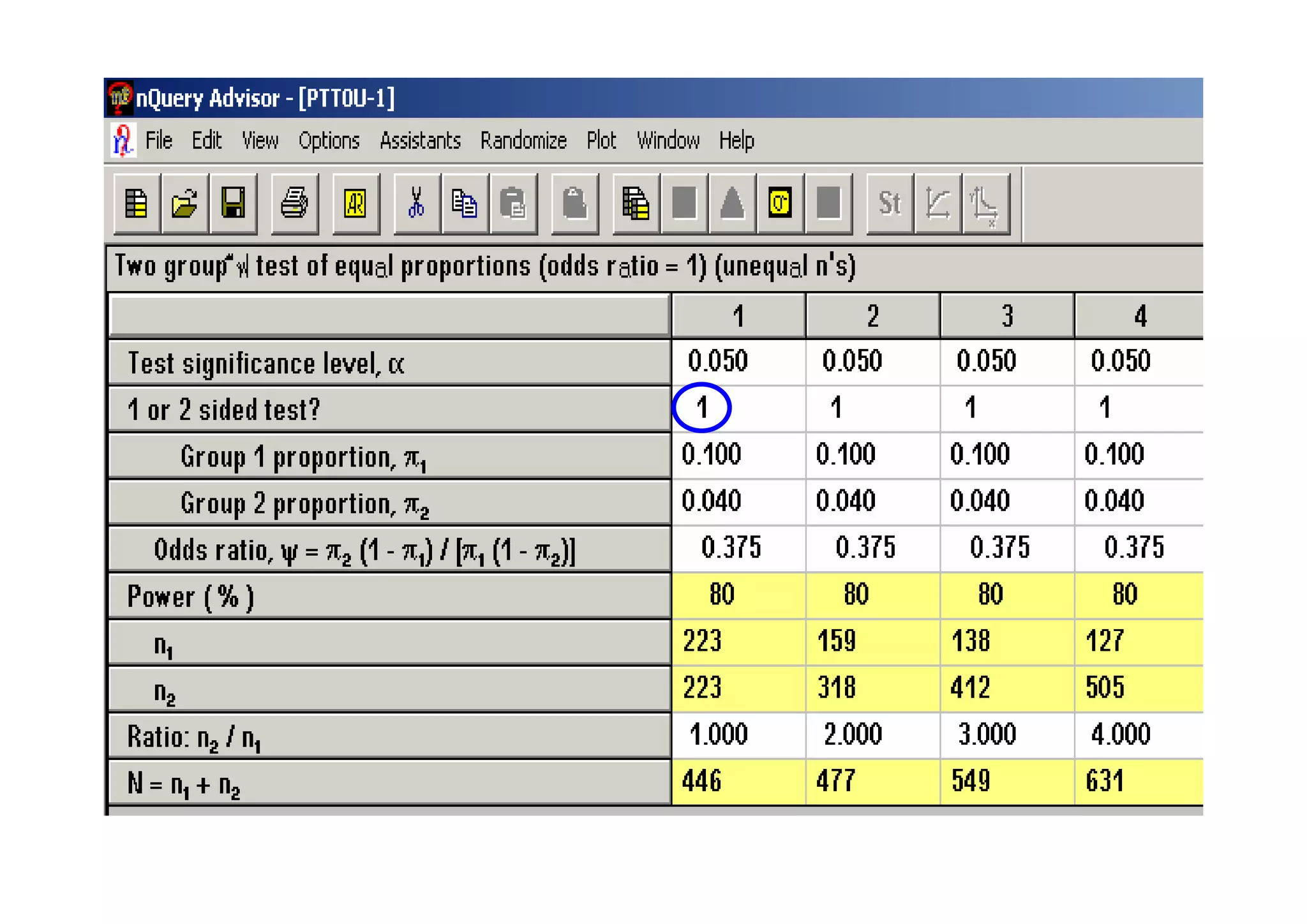
n1 = ncase= [zα/2√(r+1)pq + zβ√r p1q1 + p2q2 ]2
r (p1 – p2)2
เมื่อ
r = n2/n1 = ncontrol / ncase = 2
ิ
p1 = สัดสวนการมีประวัตการเจ็บปวยดวยโรคทางจิตในกลุม case = 0.10
q1 = 1- p1 = 0.90
ิ
p2 = สัดสวนการมีประวัตการเจ็บปวยดวยโรคทางจิตในกลุม control = 0.04
q2 = 1- p2 = 0.96
p = (p1 + rp2) / (r+1) = 0.06
q = 1- p = 0.94
α =
β =
ดังนั้น
โอกาสที่จะเกิด type I error = 0.05 (2-sided), z0.025 = 1.96
โอกาสที่จะเกิด type II error = 0.2, z0.2 = 0.842
ncase
=
[0.8062 + 0.3935]2 = 199.9
0.0072
35.
II. Test (cont’d)
2.2Test for Difference of 2 Independent Means
Example: (Aug 24, 1999, #1575)
For patients with idiopathic membranous
glomerulopathy, a phase II, randomized (1:1),
double-blind, placebo-controlled, multi-center
study of drug A will be conducted to determine efficacy.
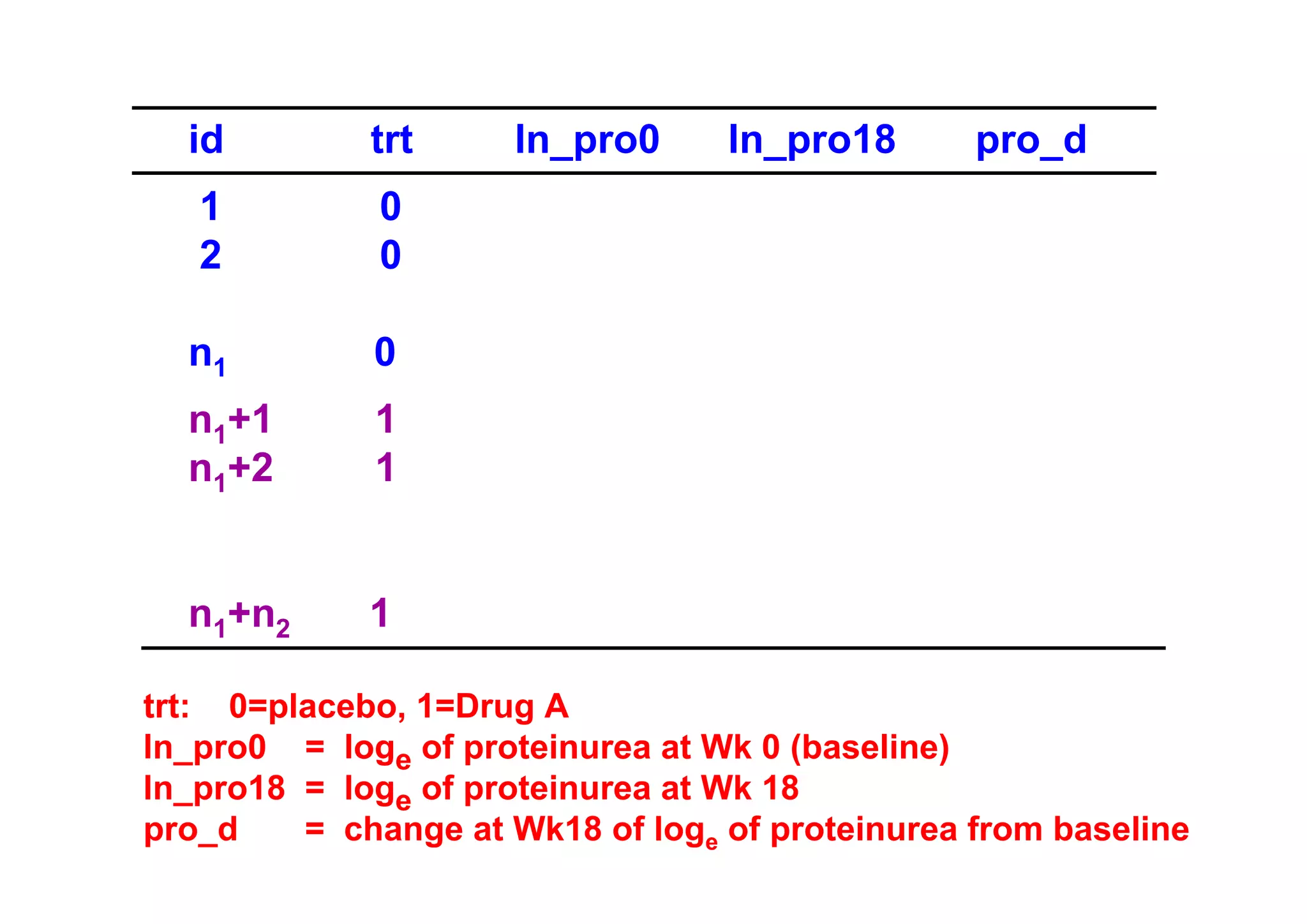
The primary efficacy endpoint is the change from
baseline in proteinuria at Week 18.
N = 45 per group will provide 80% power to detect
a difference in mean change in loge of urine protein of
–1.22 for placebo and –2.00 for an active drug,
assuming SD = 1.30, 2-sided α of 0.05.
A drop-out rate of 20% is expected, so N = 55 per group
will be recruited.
Hypotheses
or
or
H0
H1
H1
H1
:
:
:
:
μ1 - μ2
μ1- μ2
μ1 - μ2
μ1 - μ2
=
≠
>
<
0
0 (2-sided)
0 (1-sided, upper tail)
0 (1-sided, lower tail)
where μ1 = true (population) mean in group 1
μ2 = true (population) mean in group 2
38.
Zα if 1-sided
Calculation:n1 = n2 = n
n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
σ = Common standard deviation of change in
loge urine protein
= 1.30
(σ1 = σ2 = σ)
Δ = Difference in mean change between 2 groups
that is considered clinically important
= (-1.22) – (-2.00)
= 0.78
Δ / σ = Effect size (ES)
= effect of treatment in SD unit
α = 0.05 (2-sided), z0.025 = 1.96
z0.2
= 0.842
1 - β = 0.80,
where
Drop-out 20%
n / group =
n / group =
44
44
= 55
(1- dropout)
Ex:
Title: Can kneeimmobilization after total knee replacement (TKA)
save blood from wound drainage
Investigator: Dr. Vajara Wilairatana
Design:
Randomized controlled trial
Subjects:
Pts. with hip disease that require TKA
Pts. with hip disease that require TKA
Randomization
Knee elevation 40°
Blood loss
A-P splint and
Knee elevation 40°
Blood loss
41.
n/group = 2[
(zα/2 + z β )σ
Δ
]
2
where
Δ = Difference in mean postoperative blood loss
between 2 groups
σ = SD of postoperative blood loss
Kim YH et al.
Knee splint in 69 knees, mean wound drainage = 436 ml,
SD = 210 ml
Ishii et al.
30 non-splint knees, mean blood loss = 600 ml, SD = 293
42.
Ex:
Title: Early postoperativepain and urinary retention after closed
hemorrhoidectomy: Comparison between spinal and
local anesthesia
Investigator: Dr. Sahapol Anannamcharoen
Design:
RCT
Subjects:
Pts. with grade 3 or 4 hemorrhoidal disease
Pts. with hemorrhoidal disease
Randomization
Spinal anesthesia
Perianal nerve block
Visual analogue scale (VAS) pain score (0-10)
Sample size ifNon-parametric (Mann-Whitney) test is used
(VAS pain score is usually positively skewed !!)
46.
II. Test
2.4 Testof Significance of 1 Proportion
Example: (Feb 29, 2000, #1649)
N = 100 subjects with nontuberculous mycobacteria
infection will be recruited for this multi-center study.
The primary objective is to test if the frequency of
cystic fibrosis transmembrane conductance regulator
(CFTR) gene mutation is 4%. If more CF carriers are
found at a statistically significant number, then this
would suggest that CFTR alleles may be important in
predisposing to this disease.
N = 96 will provide 90% power to test H0 : π = π0 = 0.04,
against 1-sided H1 : π = π1 = 0.115, using α = 0.05.
II. Test (cont’d)
2.5Test of Significance of 1 Mean
Example:
The average weight of men over 55 years of age
with newly diagnosed heart disease was 90 kg.
However, it is suspected that the average weight is
now somewhat lower.
How large a sample would be necessary to test,
at 5% level of significance with a power of 90%,
whether the average weight is unchanged versus
the alternative that it has decreased from 90 to 85 kg
with an estimated SD of 20 kg?
n
=
(Zα/2 + Zβ)
2
+3
[F(Z0) + F(Z1)]
α = Probability of type I error = 0.05 (2-sided)
Z0.025 = 1.96
β = Probability of type II error = 0.1
1-β = Power = 0.90
Z0.1 = 1.282
F(Z)
= Fisher’s Z transformation
= 0.5 ln [(1+ρ)/(1-ρ)]
Under H0: ρ=0
F(Z0) = 0.5 x ln [(1+0)/(1-0)]
Under H1: ρ=0.3
F(Z1) = 0.5 x ln [(1+0.3)/(1-0.3)] = 0.31
Thus,
n = [ (1.96+1.282)/(0-0.31) ]2 + 3
= 112.4 = 113
= 0
54.
More than oneprimary outcome
If one of these endpoints is regarded as more important
than others, then calculate n for that primary endpoint.
If several outcomes are regarded as equally important,
then calculate n for each outcome in turn,
and select the largest n as the sample size required to
answer all the questions of interest.
55.
Caution:
Calculation of samplesize needs a number of
assumptions and ‘guesstimates’,
so such calculation only provides a guide to the
number of subjects required.
56.
Sample size estimation:
1.Formulas
2. Published tables, nomograms
3. Softwares e.g.,
- nQuery Advisor
- PS (Power and Sample Size Program)
- etc.
57.
References
Blackwelder WC. Provingthe Null Hypothesis in Clinical
Trials. Controlled Clinical Trials 1982; 3: 345-353.
Breslow NE, Day NE. Statistical Methods in Cancer
Research Vol. II – The Design and Analysis of Cohort
Studies. Oxford : Oxford University Press; 1987.
Chow SC, Liu JP. Design and Analysis of Clinical Trials.
Concept and Methodologies. New York: John Wiley & Sons,
Inc. 1998.
Fleiss JL. Statistical Methods for Rates and Proportions.
New York : John Wiley & Sons; 1981.
Karlberg J, Tsang K. Introduction to Clinical Trials: Clinical
Trials Research Methodology, Statistical Methods in Clinical
Trials, The ICH GCP Guidelines. Hong Kong: The Clinical
Trials Centre. 1998.
58.
Lachin JM. Introductionto Sample Size Determination
and Power Analysis for Clinical Trials. Controlled Clinical
Trials 1981; 2: 93-113.
Lemeshow S, Hosmer DW, Klar J, Lwanga SK.
Adequacy of Sample Size in Health Studies. New York :
John Wiley & Sons; 1990.







![Commonly used formulas: Summary
1)
Estimation
1.1) Estimate single proportion
95% CI of π = p ± d
(π = True pop’n proportion
p = Expected proportion e.g., prevalence
q = 1-p
d = Margin of error in estimating p)
2
zα/2 pq
n =
d2
1.2) Estimate single mean
95% CI of μ =⎯x ± d
(μ = True pop’n mean
⎯x = Expected mean
d = Margin of error in estimating mean)
n = [zα/2 SD / d]2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-8-320.jpg)
![2)
Test
2.1) Test of difference in 2 independent proportions (p1, p2)
p1, p2 = Proportion of … in group 1 and 2
p
= (p1+p2)/2
n/group = [
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
2.2) Test of difference in 2 independent means (Δ)
σ = Common SD of outcome var. in group 1, 2
Δ = Difference in mean b/t 2 groups
n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
2.3) Test of difference in > 2 independent means
]2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-9-320.jpg)
![2.4) Test of significance of 1 proportion
H0: π = π0
H1: π = π1
n =[
zα p 0 q 0 + z β p1q1
p 0 − p1
2.5) Test of significance of 1 mean
H0: μ = μ0
H1: μ = μ1
Δ = |μ1 - μ0|
σ = SD of outcome var.
n = [
(z α + z β )σ
Δ
]2
]2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-10-320.jpg)
![2.6) Test of significance of 1 correlation
n
F(Z)
=
=
(Zα/2 + Zβ) 2 + 3
[F(Z0) + F(Z1)]
0.5 ln [(1+ρ)/(1-ρ)]](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-11-320.jpg)






![1.3 Estimation of 1 Mean
การศึกษานี้มีวัตถุประสงคเพื่อประมาณคาเฉลี่ยของ subcarinal angle
ในคนไทยปกติ และจากการศึกษาของ ... ในคนปกติจํานวน 100 รายอายุ ... ป
พบวาคาเฉลี่ยของ subcarinal angle เทากับ 60.8 (SD=11.8)
ถากําหนดให 95% confidence interval (CI) ของคาเฉลี่ยของ
subcarinal angle ในประชากรไทย (μ) มีคาเทากับ 61 ± 2 (SD=13)
จะตองทําการศึกษาในคนไทยปกติจํานวน 163 คนดังรายละเอียดการคํานวณดังนี้
เมื่อ
ดังนั้น
n = [zα/2 SD / d]2
SD = Standard deviation ของ subcarinal angle
= 13
d = Margin of error ในการประมาณคาเฉลี่ย = 2
α = Probability of type I error (2-sided) = 0.05
z0.025 = 1.96
n = [1.96*13/2]2 = 162.31 = 163](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-18-320.jpg)







![Calculation: n1 = n2 = n
Based on Chi-square test without continuity correction
Zα if 1-sided
n/group = [
where
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
]2
p1 = response rate in group 1 = 0.07
= 0.93
q1 = 1 - p1
p2 = response rate in group 2 = 0.18
q2 = 1 – p2
= 0.82
p
q
= (p1 + p2) / 2
= 1–p
α = 0.05 (2-sided),
1- β = 0.80,
n/group = 141
= 0.125
= 0.875
z0.025 = 1.96
z0.2
= 0.842](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-26-320.jpg)



![Sample size estimation: Based on Test of 2 independent proportions
Our unit
hypothermia in low birth weight, premature infants = 55%
(p1 = 0.55)
Assume that plastic wrap would reduce hypothermia to 20%
(p2 = 0.2)
n/group = [
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
]
2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-30-320.jpg)

![n1 = ncase = [zα/2√(r+1)pq + zβ√r p1q1 + p2q2 ]2
r (p1 – p2)2
เมื่อ
r = n2/n1 = ncontrol / ncase = 2
ิ
p1 = สัดสวนการมีประวัตการเจ็บปวยดวยโรคทางจิตในกลุม case = 0.10
q1 = 1- p1 = 0.90
ิ
p2 = สัดสวนการมีประวัตการเจ็บปวยดวยโรคทางจิตในกลุม control = 0.04
q2 = 1- p2 = 0.96
p = (p1 + rp2) / (r+1) = 0.06
q = 1- p = 0.94
α =
β =
ดังนั้น
โอกาสที่จะเกิด type I error = 0.05 (2-sided), z0.025 = 1.96
โอกาสที่จะเกิด type II error = 0.2, z0.2 = 0.842
ncase
=
[0.8062 + 0.3935]2 = 199.9
0.0072](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-32-320.jpg)





![Zα if 1-sided
Calculation: n1 = n2 = n
n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
σ = Common standard deviation of change in
loge urine protein
= 1.30
(σ1 = σ2 = σ)
Δ = Difference in mean change between 2 groups
that is considered clinically important
= (-1.22) – (-2.00)
= 0.78
Δ / σ = Effect size (ES)
= effect of treatment in SD unit
α = 0.05 (2-sided), z0.025 = 1.96
z0.2
= 0.842
1 - β = 0.80,
where
Drop-out 20%
n / group =
n / group =
44
44
= 55
(1- dropout)](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-38-320.jpg)
![Δ
σ
0.78
Power
n / group
45
60
80
60
1.30
80
108
1.50
n/group = 2 [
80
90
1.50
0.50
1.30
80
143
(zα/2 + z β )σ
Δ
]2
(mean1 – mean2)
σ
Power
α
n](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-39-320.jpg)

![n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
where
Δ = Difference in mean postoperative blood loss
between 2 groups
σ = SD of postoperative blood loss
Kim YH et al.
Knee splint in 69 knees, mean wound drainage = 436 ml,
SD = 210 ml
Ishii et al.
30 non-splint knees, mean blood loss = 600 ml, SD = 293](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-41-320.jpg)





![Hypotheses
H0 : π = π0 (π0 = 0.04 )
H1 : π > π0 (π1 = 0.115)
Calculation
n =[
where
zα p 0 q 0 + z β p1q1
p 0 − p1
p0 =
q0 = 1 – p0
0.04
= 0.96
p1 =
q1 = 1 – p1
]
2
0.115
= 0.885
α = 0.05 (1-sided), z0.05 = 1.645
1- β = 0.90,
z0.1 = 1.282
n = 96](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-47-320.jpg)

![Hypotheses
H0 : μ = μ0 (μ0 = 90)
H1 : μ < μ0 (μ1 = 85)
Calculation
n = [
where
(z α + z β )σ
Δ
σ = estimated SD
Δ = | μ1 - μ0|
]
2
= 20
= 5
α = 0.05 (1-sided), z0.05 = 1.645
1- β = 0.90,
z0.1 = 1.282
n = 137.08 = 138](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-49-320.jpg)


![n
=
(Zα/2 + Zβ)
2
+ 3
[F(Z0) + F(Z1)]
α = Probability of type I error = 0.05 (2-sided)
Z0.025 = 1.96
β = Probability of type II error = 0.1
1-β = Power = 0.90
Z0.1 = 1.282
F(Z)
= Fisher’s Z transformation
= 0.5 ln [(1+ρ)/(1-ρ)]
Under H0: ρ=0
F(Z0) = 0.5 x ln [(1+0)/(1-0)]
Under H1: ρ=0.3
F(Z1) = 0.5 x ln [(1+0.3)/(1-0.3)] = 0.31
Thus,
n = [ (1.96+1.282)/(0-0.31) ]2 + 3
= 112.4 = 113
= 0](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/85/Sample-size-estimation-52-320.jpg)













![Commonly used formulas: Summary
1)
Estimation
1.1) Estimate single proportion
95% CI of π = p ± d
(π = True pop’n proportion
p = Expected proportion e.g., prevalence
q = 1-p
d = Margin of error in estimating p)
2
zα/2 pq
n =
d2
1.2) Estimate single mean
95% CI of μ =⎯x ± d
(μ = True pop’n mean
⎯x = Expected mean
d = Margin of error in estimating mean)
n = [zα/2 SD / d]2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-8-2048.jpg)
![2)
Test
2.1) Test of difference in 2 independent proportions (p1, p2)
p1, p2 = Proportion of … in group 1 and 2
p
= (p1+p2)/2
n/group = [
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
2.2) Test of difference in 2 independent means (Δ)
σ = Common SD of outcome var. in group 1, 2
Δ = Difference in mean b/t 2 groups
n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
2.3) Test of difference in > 2 independent means
]2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-9-2048.jpg)
![2.4) Test of significance of 1 proportion
H0: π = π0
H1: π = π1
n =[
zα p 0 q 0 + z β p1q1
p 0 − p1
2.5) Test of significance of 1 mean
H0: μ = μ0
H1: μ = μ1
Δ = |μ1 - μ0|
σ = SD of outcome var.
n = [
(z α + z β )σ
Δ
]2
]2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-10-2048.jpg)
![2.6) Test of significance of 1 correlation
n
F(Z)
=
=
(Zα/2 + Zβ) 2 + 3
[F(Z0) + F(Z1)]
0.5 ln [(1+ρ)/(1-ρ)]](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-11-2048.jpg)





![1.3 Estimation of 1 Mean
การศึกษานี้มีวัตถุประสงคเพื่อประมาณคาเฉลี่ยของ subcarinal angle
ในคนไทยปกติ และจากการศึกษาของ ... ในคนปกติจํานวน 100 รายอายุ ... ป
พบวาคาเฉลี่ยของ subcarinal angle เทากับ 60.8 (SD=11.8)
ถากําหนดให 95% confidence interval (CI) ของคาเฉลี่ยของ
subcarinal angle ในประชากรไทย (μ) มีคาเทากับ 61 ± 2 (SD=13)
จะตองทําการศึกษาในคนไทยปกติจํานวน 163 คนดังรายละเอียดการคํานวณดังนี้
เมื่อ
ดังนั้น
n = [zα/2 SD / d]2
SD = Standard deviation ของ subcarinal angle
= 13
d = Margin of error ในการประมาณคาเฉลี่ย = 2
α = Probability of type I error (2-sided) = 0.05
z0.025 = 1.96
n = [1.96*13/2]2 = 162.31 = 163](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-18-2048.jpg)






![Calculation: n1 = n2 = n
Based on Chi-square test without continuity correction
Zα if 1-sided
n/group = [
where
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
]2
p1 = response rate in group 1 = 0.07
= 0.93
q1 = 1 - p1
p2 = response rate in group 2 = 0.18
q2 = 1 – p2
= 0.82
p
q
= (p1 + p2) / 2
= 1–p
α = 0.05 (2-sided),
1- β = 0.80,
n/group = 141
= 0.125
= 0.875
z0.025 = 1.96
z0.2
= 0.842](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-26-2048.jpg)



![Sample size estimation: Based on Test of 2 independent proportions
Our unit
hypothermia in low birth weight, premature infants = 55%
(p1 = 0.55)
Assume that plastic wrap would reduce hypothermia to 20%
(p2 = 0.2)
n/group = [
zα/2 2pq + z β p1q1 + p 2 q 2
p1 − p 2
]
2](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-30-2048.jpg)
![n1 = ncase = [zα/2√(r+1)pq + zβ√r p1q1 + p2q2 ]2
r (p1 – p2)2
เมื่อ
r = n2/n1 = ncontrol / ncase = 2
ิ
p1 = สัดสวนการมีประวัตการเจ็บปวยดวยโรคทางจิตในกลุม case = 0.10
q1 = 1- p1 = 0.90
ิ
p2 = สัดสวนการมีประวัตการเจ็บปวยดวยโรคทางจิตในกลุม control = 0.04
q2 = 1- p2 = 0.96
p = (p1 + rp2) / (r+1) = 0.06
q = 1- p = 0.94
α =
β =
ดังนั้น
โอกาสที่จะเกิด type I error = 0.05 (2-sided), z0.025 = 1.96
โอกาสที่จะเกิด type II error = 0.2, z0.2 = 0.842
ncase
=
[0.8062 + 0.3935]2 = 199.9
0.0072](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-32-2048.jpg)



![Zα if 1-sided
Calculation: n1 = n2 = n
n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
σ = Common standard deviation of change in
loge urine protein
= 1.30
(σ1 = σ2 = σ)
Δ = Difference in mean change between 2 groups
that is considered clinically important
= (-1.22) – (-2.00)
= 0.78
Δ / σ = Effect size (ES)
= effect of treatment in SD unit
α = 0.05 (2-sided), z0.025 = 1.96
z0.2
= 0.842
1 - β = 0.80,
where
Drop-out 20%
n / group =
n / group =
44
44
= 55
(1- dropout)](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-38-2048.jpg)
![Δ
σ
0.78
Power
n / group
45
60
80
60
1.30
80
108
1.50
n/group = 2 [
80
90
1.50
0.50
1.30
80
143
(zα/2 + z β )σ
Δ
]2
(mean1 – mean2)
σ
Power
α
n](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-39-2048.jpg)

![n/group = 2 [
(zα/2 + z β )σ
Δ
]
2
where
Δ = Difference in mean postoperative blood loss
between 2 groups
σ = SD of postoperative blood loss
Kim YH et al.
Knee splint in 69 knees, mean wound drainage = 436 ml,
SD = 210 ml
Ishii et al.
30 non-splint knees, mean blood loss = 600 ml, SD = 293](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-41-2048.jpg)





![Hypotheses
H0 : π = π0 (π0 = 0.04 )
H1 : π > π0 (π1 = 0.115)
Calculation
n =[
where
zα p 0 q 0 + z β p1q1
p 0 − p1
p0 =
q0 = 1 – p0
0.04
= 0.96
p1 =
q1 = 1 – p1
]
2
0.115
= 0.885
α = 0.05 (1-sided), z0.05 = 1.645
1- β = 0.90,
z0.1 = 1.282
n = 96](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-47-2048.jpg)

![Hypotheses
H0 : μ = μ0 (μ0 = 90)
H1 : μ < μ0 (μ1 = 85)
Calculation
n = [
where
(z α + z β )σ
Δ
σ = estimated SD
Δ = | μ1 - μ0|
]
2
= 20
= 5
α = 0.05 (1-sided), z0.05 = 1.645
1- β = 0.90,
z0.1 = 1.282
n = 137.08 = 138](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-49-2048.jpg)


![n
=
(Zα/2 + Zβ)
2
+ 3
[F(Z0) + F(Z1)]
α = Probability of type I error = 0.05 (2-sided)
Z0.025 = 1.96
β = Probability of type II error = 0.1
1-β = Power = 0.90
Z0.1 = 1.282
F(Z)
= Fisher’s Z transformation
= 0.5 ln [(1+ρ)/(1-ρ)]
Under H0: ρ=0
F(Z0) = 0.5 x ln [(1+0)/(1-0)]
Under H1: ρ=0.3
F(Z1) = 0.5 x ln [(1+0.3)/(1-0.3)] = 0.31
Thus,
n = [ (1.96+1.282)/(0-0.31) ]2 + 3
= 112.4 = 113
= 0](https://image.slidesharecdn.com/samplesizeestimation-140124125726-phpapp02/75/Sample-size-estimation-52-2048.jpg)