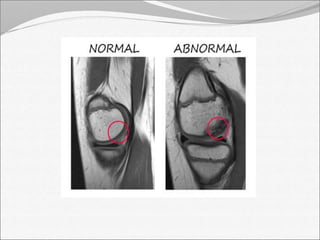
This document discusses the causes, risk factors, and clinical manifestations of septic arthritis. It causes include bacteria, viruses, mycobacteria, and fungi. Risk factors include rheumatoid arthritis, IV drug use, immunosuppression, diabetes, and age over 80. Symptoms include fever, severe pain, swelling, tenderness, and limited mobility in the affected joint. Imaging plays an important role in diagnosis, with ultrasound, CT, MRI, and nuclear medicine scans able to detect infection earlier than plain x-rays. Complications can include bone and cartilage destruction, joint fibrosis or ankylosis, and growth disturbances in children.