This document discusses various complications that can arise regarding the mother and passenger (baby) during pregnancy and childbirth. It covers complications such as prolapse of the umbilical cord, multiple gestation, fetal positioning issues like face presentation and brow presentation, fetal size issues like macrosomia and shoulder dystocia, and breech presentation. It also discusses managing the mother's psyche and emotional state during birth as that can impact the birthing process if she is feeling afraid, tense or unsupported. Effective management strategies are provided for each complication depending on whether a normal spontaneous delivery is possible or if cesarean section is required.
NCM 109- Careof Mother
and Child at Risk or with
Problems
(Acute and Chronic)-LECTURE
Wesleyan University –Philippines
Cabanatuan City
CONAMS
Jhonee Balmeo
Instructor
2.
YEIZ! this wouldbe the baby!
Since the mother carries the
baby in her body, hence the
term passenger.
Complications
to Passenger
3.
III. Complications withthe Passenger
1.Prolapse of the Umbilical Cord
A loop of the umbilical cord slips down in
front of the presenting fetal part.
If the presenting fetal part is not fitted firmly
into the cervix
Occur after rupture of membrane
The pressure of the fetal head against the
cord at the pelvic brim leads to cord
compression and decreased oxygenation to
the fetus
Management:
Goal: relieving pressureon the cord, to
relieve pressure the compression and
the resulting fetal anoxia
Procedure:
1.Placing a gloved hand in the vagina
and manually elevating the fetal head
off the cord
7.
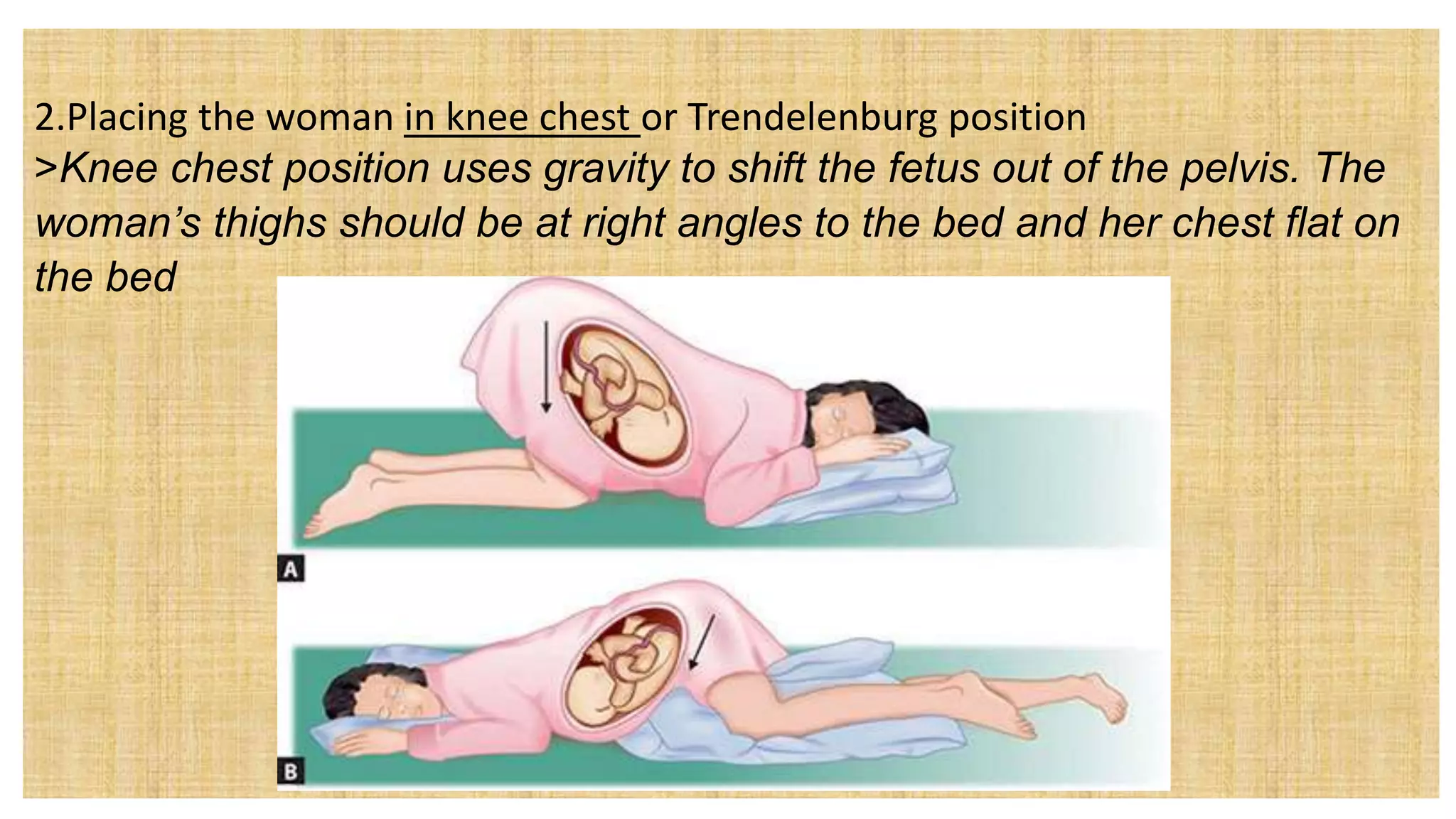
2.Placing the womanin knee chest or Trendelenburg position
>Knee chest position uses gravity to shift the fetus out of the pelvis. The
woman’s thighs should be at right angles to the bed and her chest flat on
the bed
8.
3. Administer Oxygenby mask
10L/min by face mask to the woman-
helpful to improve oxygenation to the
fetus.
4. Do not attempt to push any exposed
cord back into vagina-this can cause
more compression by knotting or
kinking
5.Cover any exposed portion with a
sterile saline compress to prevent
drying.
6. Cesarean Birth-if no cervical
dilatation
Management:
1.If NSD:
Instruct womanto come to the
hospital early in labor
First stage may be long
Urge woman to spend the early
hours in an activity to make time
pass more quickly
Teach woman proper breathing
techniques or exercises
During labor- support the woman’s
breathing pattern- to minimize the
use of analgesia and minimize any
respiratory difficulties among infants
11.
Management:
1.If NSD:
Expect tohear two separate beats as
proof each infant is doing well
Expect for abnormal presentation may
occur-vertex and breech
Expect head engagement may not occur
because the babies are usually small-cord
prolapse after rupture of membrane
Expect uterine dysfunction, overstretched
uterus, unusual presentation and
premature separation of the placenta after
birth of the first child
12.
The first infantis identified as A, immediately
newborn care is given.
Oxytocin is not given yet after the delivery of the
first infant-to avoid compromising the circulation
of the infants not yet born
Assess woman for post partum hemorrhage and
infection due to prolonged labor
13.
2.If by C/S:
Additionalpersonnel are needed
Focus on the woman’s needs as
well as those of her babies
Prepare pre operative
management
14.
Problems with fetalposition, presentation, or size
1.Face presentation
A fetal head presenting at a different angle than expected is termed asynclitism
• Asynclitism is defined as the "oblique malpresentation of the fetal head in
labor".
Example: face and brow presentations
*face (chin or or mentum) is rare, but when it does occur, the head diameter the fetus
presents on the pelvis is often too large for birth to proceed.
15.
Signs and Symptoms:
Headfeels more prominent than normal
No engagement apparent on Leopold’s
maneuvers,
Present with contracted uterus or placenta previa,
polyhydramnios, or fetal malformation
Diagnosis: assessment thru:
Palpation: vaginal examination – when nose,
mouth or chin can be felt
UTZ
16.
What to expectfrom an Infant:
Facial edema
Purple from ecchymotic bruising
Observe infant for patent airway
17.
TRY NATIN SAGUTINITO…
Bruh! Lam mo bang Mas Malaki ang chance for multiple gestation if…
•A. kung ang edad mo ay more than 30 na (malapit ng mawala sa calendar bruh)
•B. you’re taking fertility drugs
•C. sa family mo, may history talaga ng multiple gestation
•D. lahat ng nabanggit ni sheer…
18.
BASICS!
You were assignedin the ICU and was assigned to measure
the head circumference of the infant. You would most
appropriately:
A. Wrap the tape measure around the infant’s head and
measure just above the eyebrows.
B. Place the tape measure under the infant's head at the base
of the skull and wrap around to the front just above the
eyes
C. Place the tape measure under the infant's head, wrap
around the occiput, and measure just above the eyes.
D. Place the tape measure at the back of the infant’s head,
wrap around across the ears, and measure across the
19.
b. Brow presentation
Therarest of the presentation
Occurs in multipara or with woman with relaxed abdominal mucles
Can results to obstructed labor due to head becomes jammed in the brim of
the perlvis
Management: C/S
20.
b. Brow presentation
Therarest of the presentation
Occurs in multipara or with woman with relaxed abdominal mucles
Can results to obstructed labor due to head becomes jammed in the brim of the perlvis
Management: C/S
21.
c. Transverse Lie
Occursin women with pendulous abdomen,
uterine fibroid tumors
Contractions of the pelvic brim, with congenital
anomalies of the uterus, or with polyhydramnios
Occur in infants with hydrocephalus or any
abnormality that prevents the head from
engaging
May occur in prematurity if the infant has room
for free movement
22.
Diagnosis thru assessment:
method:inspection: the ovoid of the
uterus is found to be more horizontal
than vertical
Can be confirmed by LM
UTZ for final confirmation
Management: a mature infant cannot
be born normally: membranes rupture
prematurely, cord or arm can prolapse,
or shoulder may obstruct the cervix
> C/S
23.
d. Macrosomia
Weighs morethan 4,000 to 4,500 g (9-10 lbs)
High incidence: women with diabetes or who developed gestational diabetes
Risk:
• uterine dysfunction due to overstretching of the uterus
• Fetal pelvic disproportion – due to the wide shoulders of the infant
• Perineal lacerations
Management: C/S
24.
Fetal Risks:
>Brachial plexus injury
o The brachial plexus is the network of nerves that sends signals from your spinal cord
to your shoulder, arm and hand.
o A brachial plexus injury occurs when these nerves are stretched, compressed, or in
the most serious cases, ripped apart or torn away from the spinal cord.
o Due to improper or excessive traction applied to the fetal head
• Brachial plexus injuries during childbirth include:
25.
Erb-Duchenne Palsy
– >It involves injury to the 5th, 6th and sometimes the 7th cervical nerve roots. It
results in paralysis of the deltoid and infraspinatus muscles as well as the flexor
muscles of the forearm.
– > The affected extremity is held straight and internally rotated with the elbow
extended and the wrist and fingers flexed.
– > Moro, biceps and radial reflexes are
absent on the affected extremity however,
grasp reflex remains intact.
e.Shoulder Dystocia
Problem occursat 2nd stage of labor- fetal head is born but the shoulders are too
broad to enter and be born through the pelvic outlet
Danger:
a. hazardous to the woman- can cause vaginal or cervical tears
b. Hazardous to the infant-if cord is compressed between the body and the bony
pelvis
Common in:
> Women with diabetes, multiparas, postdate pregnancies
Diagnosis: if 2nd stage is prolonged: arrest of descent,
head appears in the perineum (crowning)
f. Breech Presentation
>when the fetus presents buttocks or feet first (rather than head first – a
cephalic presentation).
Complication to be anticipated:
> Perinatal morbidity and mortality from difficult delivery
>LBW from prematurity, growth retardation
>Prolapsed cord
>Placenta previa
>Multiple fetuses
3. Footling breech– one or both feet is
at the lowermost in the birth canal
33.
Diagnosis:
1. Abdominal exam– leopold’s maneuver
LM1 – hard, round, readily ballotable fetal head is found to occupy the fundus
34.
LM 2 –indicates the back to be on one side of the abdomen and the small parts on
the other
LM3 – breech is movable above the pelvic inlet
LM4 – firm breech to be beneath the symphysis
• FHB is in the lower quadrant and/or in the umbilicus
2. Vaginal exam – both ischial, sacrum and the anus are palpable
3. x-ray and ultrasound
35.
BASICS!
Bruh! You areassessing the bagong tuli na infant, you just
noticed that the circumcised area is namumula at may small
amount of bloody drainage. Bilang isang malufet na nurse,
which of the following nursing actions would be most
appropriate?
A. Document the findings
B. Contact the physician
C. Circle the amount of bloody drainage on the dressing and
reassess in 30 minutes
D. Reinforce the dressing
36.
IV. Complications withthe Psyche
> It is another word for you your emotional state during
birth.
• A good emotional state helps mom cope with the pain
effectively;
• helps her tune in to her body;
• helps guide her to her baby’s needs and allows the other
3 P’s to sync up effectively
37.
IV. Complications withthe Psyche
If mom is afraid, tense, stressed out,
angry, feels unsafe or unsupported,
she will not likely do well during birth.
For some, the fear is intense enough
to schedule a c-section and to avoid a
vaginal birth all together.
For others, it may prevent cervical
dilation, fetal decent, or prevent mom
from pushing effectively.
Uwu!!!